71,036 views | 01:06:47

![]()








We have fallen woefully behind in the race to keep up with harmful bacteria as they continually evolve to outsmart our antibiotics, in fact, there are already superbugs we cannot defeat. Predictions are by 2050 there will be more deaths from infections than from cancer if we don’t solve this crisis. Join immunologists, biologists, and infectious disease specialists to explore some exciting new tools that may be our salvation in the battle against superbugs.
This program is part of the Big Ideas Series, made possible with support from the John Templeton Foundation.
CARL ZIMMER: Thank you all for coming. Tonight we’re going to talk about a very serious subject. Um, the situation that we face with antibiotic resistant bacteria. Antibiotics were once the silver bullet that seemed to be able to cure just about everything. Now we look at 23,000 antibiotic resistant bacterial infections every year. So let me introduce you to our panelists. Our first participant is the Director of the Wisconsin Institute for Discovery at the University of Wisconsin-Madison. She was a science advisor to President Barack Obama. Please welcome Jo Handelsman. Our next participant is a professor at Rockefeller University where he is head of the Laboratory of Bacterial Pathogenesis and Immunology. Please welcome Vincent Fischetti.
ZIMMER: Our next participant is an associate professor of Immunobiology and Microbial Pathogenesis at The Salk Institute. Please welcome Janelle Ayres.
ZIMMER: Our next participant is the Evnin Associate Professor at Rockefeller University. Please welcome Sean Brady.
ZIMMER: and finally the Singer Professor of Medicine in Microbiology, and the Director of the Human Microbiome Program at NYU School of Medicine. Please welcome Martin Blaser.
ZIMMER: Uh so, I thought that maybe a way to start would be to show a video. This was an experiment that was done at Harvard where basically scientists created at sort of gigantic petri dish, sort of kind of the size of an air hockey table basically, and they seeded it with bacteria on either side and then basically laced it with antibiotics. Starting at the edge with pretty mild levels and then as you go further in, it gets more and more deadly until the central band has a thousand times the lethal dose for Ecoli. It’s really kind of mind blowing. We’re going to see the bacteria, so just sort of hanging out there and now they’re multiplying. This is sort of time lapse, so when they hit that point, what they’re encountering that as antibiotics and then how are they getting past it? I mean you can see them.
JO HANDELSMAN: It takes a little bit of time and what they’re waiting for is growth of one or a very small number of cells in the population that are already resistant. And so although there were many, many billions of cells crossing the plate, probably one in a million would have resistance to the antibiotic, so once those started dividing and-
ZIMMER: So they’re dividing and one in a million just happens to gain this power to get past it?
HANDELSMAN: Well, they always had the power. It was preexisting in the population, but then when the whole population is, the rest of the population is stopped by the antibiotic because they’re inhibited by it. Then those few that are resistant start proliferating and then they take over and that’s exactly what it looks like in similar terms when it’s in the body, you know, you take an antibiotic and most of the bacteria will die, but there will be preexisting mutants in the population that are resistant.
ZIMMER: That’s great. Well not great, but it’s amazing.
HANDELSMAN: It is definitely not great.
ZIMMER: Yeah, no it didn’t. I know, I know. Don’t get me wrong. We think of antibiotics as, as the sort of heroic triumph of science. I mean, how did, how did we get to enjoy the benefits of antibiotics? I mean, how did that begin?
HANDELSMAN: Well, it started with a chance discovery from a by Sir Alexander Fleming. In the UK, who found a fungus on his plate that was clearly inhibiting growth of staphylococcus on, on the Petri dish, and he recognized what it was that this was a compound that was diffusing into the Auger and determined that it was what we now know of as penicillin, but it was many years before it can be used in any kind of broad scale way because he discovered that in 1929 and by the start of World War II, we still, we’re not using antibiotics and they weren’t in general use.
ZIMMER: Why not? I mean you, you discover a drug, you know, put it into practice. I mean, what was the holdup?
HANDELSMAN: They couldn’t make enough of it. That fungus produced some but not enough to go into large scale production. And so during the war a scientist named Ken Raper was worked for the USDA in Peoria and he decided as a war effort to put out the call for penicillin producing strains of penicillium mold. So he told everybody in Peoria to collect as many fruits and vegetables with that green blue fuzzy thing that you see on your bread and fruit to bring those to his lab. And people did and he had this large collection and it turned out it was his own technician who has gone down in history, as Moldy Mary now. Her name was actually Mary Hunt and she brought in the winning cantaloupe and it had a strain of penicillium mold that produces more penicillin than any other natural strain to this day. And so they started, they moved it right into commercial production and started pumping out large amounts of penicillin and they have enough to be able to ship it the penicillin to the troops in Europe. And so World War Two was the first war in which more people died directly of bullets and bombs than the infections that accompanied them.
ZIMMER: Wow. So, and then once, once the war is over, then antibiotic start to become more of just a general medicine for the public in general, right?
HANDELSMAN: Yeah. And at the same time there was interest in soil bacteria that produced antibiotics. And, and then after the war there was just this explosion of knowledge of people, culturing organisms from the soil, screening them for antibiotics and then moving into production. And so we had dozens of antibiotics coming onto the market in the next decades.
ZIMMER: Sean, I mean, how would you sort of describe like the sort of, the overall benefit of these discoveries of penicillin and some of these other early antibiotics? I mean, what I mean overall, like in terms of lives saved or someone, what are we looking at in terms of the scale of this?
BRADY: I think one of the figures that penicillin alone has saved 100 million lives.
ZIMMER: And that’s penicillin alone.
BRADY: Yeah. So if you think about that single picture that Joe talked to you, you see it in almost any microbiology textbook. That image has probably saved more lives than anything in the history of science. So you want one kind of thing in your office, you should hang that picture as a scientist because it’s made a larger impact on human health than anything but, but that, that whole discovery, even today we’re still using those antibiotics. So. So that’s the initial discovery, then you think about almost everything that came out of what we call the golden age of antibiotics, the forties, fifties, and sixties.
ZIMMER: So people were finding things not just on cantaloupe but in other-
BRADY: They are culturing soil bacteria largely and finding antibiotics. Almost every class of antibiotics that we use today was discovered in that that time period. We have relied on antibiotic defense really of those molecules and continually using versions of those molecules up until today. And that’s why we’re in the position we are today. We, we’ve largely ceased discovering antibiotics after the golden age, the late sixties, early seventies. Because we thought we were done. We thought we had solutions to these problems. That’s how good those initial discoveries were. How, how much of an impact they made on human health.
ZIMMER: What’s your sense of like when it started to become clear that things weren’t going so well? Like when? When do you think that the sort of scientific medical community said, I think we have a problem?
BLASER: Well that happened pretty quickly. I mean we were seeing resistant organisms to penicillin early on. It was, it started
ZIMMER: Like a matter of a few years after?
BLASER: Probably a year or two
ZIMMER: After the introduction of penicillin.
BLASER: Exactly we already started to see early stages of resistance, but you know, was it an organism here, an organism there, but, but it was occurring at that time and it’s been occurring at an accelerated rate since then.
ZIMMER: Right. So Marty, what do you think is, what would you say would be like one of the main factors that explain sort of how we got to this point in terms of resistance? Like what are we doing that is causing all of these bacteria now to be just so dangerous?
BLASER: So, uh, the short answer is that Darwin was right and that is that there is survival of the fittest. It’s selection. We are using antibiotics in such magnitude because of the miraculous nature of antibiotics, both the public and the profession says, well, why don’t we just treat this person with antibiotics even if their symptoms are minimal. So there’s enormous pressure, selective pressure of antibiotic use and it’s just, it’s just a mathematical certainty that there’ll be resistance, but it’s not linear. It’s, it’s geometric because of the properties of bacteria growing.
FISCHETTI: Yes, but you have to remember that bacteria come, most of them come from the soil and antibiotics are in the soil, so they’ve learned for millions of years how to deal with antibiotics. So the systems are there for as long as you. If you expose them to antibiotics, those systems become heightened, then become resistant. So they, they’ve seen these drugs or similar drugs or antibiotics type molecules for hundreds and hundreds of thousands, millions of years.
ZIMMER: Marty, you, you’ve also been talking a lot and writing a lot about the fact that our antibiotics are not precision weapons that you know, you use them against Ecoli, MRSA, and so on, but that’s not the only thing that’s going to affect.
BLASER: Yeah, so so antibiotics came of age when we were, when we were really trying to eliminate these bad pathogens, but no one really considered what was the effect of the antibiotics or the normal bacteria living in the body, the normal bacteria that we call the microbiome, but now it’s clear that that when you take an antibiotic for a skin infection or lung or urinary tract infection, that antibiotic is getting everywhere in the body and it is selecting for resistant organisms in that body. That’s suppressing some organisms and other organisms are coming up and maybe some organisms are becoming extinct as well.
ZIMMER: So these are organisms that we might actually depend on. It might be actually beneficial for us.
BLASER: And so in fact we know that one of the main defenses against infection are our residual. Our normal organisms there, there, there, the coast guard, they are protecting against invaders. They don’t want to share their turf and 50 years ago it was shown that if you pretreat mice or other laboratory animals with antibiotics and then give them a pathogen like Salmonella, the, the level of Salmonella that it takes to kill the mouse goes down by four logs, you know, by 10,000 falls.
ZIMMER: So Sean, I mean someone might say like, well we have all these gigantic pharmaceutical companies. There’s lots of money that they can throw at the problem. You know, there was penicillin and then there were other things I can think of mycin and you know, you know, science marches on. So we’ve got like more in the pipeline, right?
BRADY: That’s the unfortunate thing. We have almost nothing in the pipeline.
ZIMMER: Almost nothing.
BRADY: You can, you can ascribe that to a number of different reasons. We don’t get in a crisis because of one thing, but we get in it because many things came together that we probably didn’t foresee. One of them being that our first round of antibiotics worked so well right? That golden age of antibiotics when we were describing them, people thought we were done and so so over the next ensuing 30 years antibody discovery programs, both in academic and industrial settings largely shut down and so there are almost no pharmaceutical industries that are putting at least the effort they used to put in to finding antibiotics. The second thing is then if we’d been using antibiotics, the same ones for 30 years, that means they don’t cost us anything anymore. They’re all generics. You can get an antibiotic for somewhere between free and twenty cents a day in many parts of the world, so now you have an infrastructure that doesn’t exist and you have a financial structure that doesn’t support the development of antibiotics. So we are at a certain point trying to figure out how to restart that pharmaceutical industry and how to make it worthwhile to restart it. Have to be some major things changed.
HANDELSMAN: It’s in direct competition with chronic disease which is much more lucrative for the companies because it drug you take for the rest of your life is obviously going to make them more money than a drug you take for five days and then stop, and so even even now with the crisis that we all know we’re in, very few companies want to move back into that area.
FISCHETTI: And what they’re doing is taking a drug that worked, became, an organism, becomes resistant, and they just make a modification on that drug. It’s cheaper for them to do that than to start from the beginning and now the virus can become resistant much more rapidly. So they work for maybe a year or two and then they can’t use them anymore.
ZIMMER: Marty.
BLASER: And then there’s yet another problem and that is that bacteria don’t respect borders and so what that means is that if, if a resistant organism arises in another country like India or China, it doesn’t take too long for it to come over here and because antibiotics are so inexpensive and because people think that they’re so miraculous. In many of these countries, people are able to get antibiotics over the counter, no prescription necessary. Parents are giving their kids 10 courses of antibiotics a year in, in some recent studies funded by the Gates Foundation, tremendous antibiotic pressure, very low cost, but somebody’s making money on those antibiotics. Resistant organisms are arising and then there are the crossing all over the world,
ZIMMER: So this, so this sort of cheap marketplace of antibiotics over the counter and so on is even helping to drive on-
BLASER: The whole antibiotic market is broken. Antibiotics are in one sense too cheap and and, and are therefore overused and abused. And on the other hand there’s no incentive to create new antibiotics that we want to keep and put in reserve for important infections, which won’t affect tens of millions of people so that there isn’t that market. So the market, the economic model for antibiotics is just broken.
BRADY: Just, just to put a number on that, right? Yeah. So the most recent, they’re going to differ a little bit, but let’s say the six months, recent antibiotics that came to market made about $10,000,000 each last year. 10, 10 million each. Right? Okay, that seems like a lot of money, but just let’s say you’ve done all the clinical trials you need and now you need to synthesize a production scale an antibiotic. It’s $150,000,000 investment, right? And the reason these things make a little money is, is you don’t want to use them. You don’t want to use in this frontline defense, right? You want to put them in reserve until you absolutely need them. And so where’s the incentive? If, if forget the hundreds of millions you put into development, just to make the thing costs you 10 times which you can sell it for, sell it for a year. We really have to rethink how we, how we market these things, how we as a community decide we’re going to put antibiotics in reserve and put an upfront and of realization that these things are there. We need to pay for them as a community because we’re going to need them some day.
ZIMMER: Alright, so let’s, let’s brighten things up a bit by like actually, you know, you folks are actually working on things. So maybe we’ll start. We’ll start with antibiotics themselves, with new antibiotics. So with Jo and Sean’s work. So, so, so you’ve been going back to the soil, the soil that brought us all these original drugs. You think you think there are more there for us to find?
HANDELSMAN: I do. I’m so, for a long time I went to other methods for antibiotic discovery and you’ll hear about some of those that Sean’s developed soon, but the reason I did that was that there were some references from the nineties that said that the soil was mined. It was fully tapped and I’ve gone back to the data and I can’t find the data and so now I question whether that’s really true because in the ensuing decades my lab just spontaneously discovered antibiotics, novel antibiotics from soil that hadn’t been discovered and we weren’t even looking in some cases. And so I. It just occurred to me one day, wait a minute, it’s not mined if we’re finding them and so that’s the approach we’re taking is going back and asking what is the frequency of new compounds? There was one paper that said the rediscovery rate would be 99 percent, so if you found 100 compounds, 99 of them would be already known. Well that’s actually not so bad if it’s true because we can look at a lot more than 100 compounds with today’s methods, but. But I’m not even sure that that’s true because it wasn’t really based on at least published data. Maybe somebody in a pharmaceutical company has the data, but we haven’t seen it.
ZIMMER: So are there particular places that you like to go look for new antibiotics? In a particular soil that is you like or is it just in your backyard?
HANDELSMAN: Well, we’re looking at across the world, so we have a worldwide network of undergraduate students. Undergraduates who are a fantastic and very creative workforce. So we developed a course that is known as the Small World Initiative and it’s taught in 15 countries and all over the United States and about 10,000 students a year take the course and they dig up soil from whatever environment is interesting to them and they come up with more interesting reasons than I ever would for why an environment is interesting. And and so they have this great variety of soils. They’re isolating very interesting antibiotic producing organisms and now we have to go into the next stage which is figuring out what antibiotics are produced. So we think that if we have 10,000 students, each one gets at least 10 antibiotic producing organisms per year. That’s a lot of candidates. And so if we can crank through enough of them, even if that one percent rediscovery or 99 percent rediscovery rate is correct, we still have a lot of new compounds to look at.
ZIMMER: So Sean, what kind of approach are you taking to searching for these, these new antibiotics?
BRADY: So about 20 years ago now, I guess, Jo and a few other people were thinking along these ideas, thinking about is there a reservoir in soil still of, of natural products and, and the thing that that percolated to the top of the thinking of these people was that there’s data from even longer ago, maybe 120 years ago that it appears we don’t culture most of the bacteria out of the environment, that actually the bugs we’ve been playing with represent a small fraction of the bacteria in the environment.
ZIMMER: So let me ask you, so if you like take a sample of a little sample of soil, first of all, like how many microbes are in there and how much DNA are you talking about that you’re looking at from all of them?
BRADY: So it depends on whose numbers, let’s say is there’s thousands, maybe 10,000 different microbes of which we culture about one percent.
ZIMMER: Just one percent,.
BRADY: Just one percent. And again, people have done better nowadays, but they don’t solve the other problem, which is even if we can culture bacteria, we don’t turn on their genes. Right? So even if you can bring bacteria in the lab, they don’t know how to turn on the genes, they’re gonna make antibiotics for us. And so, so what we want to do is just look at their DNA and you can get huge amounts of DNA at least in the context of molecular biology out of a single gram of soil.
BRADY: And so it’s the coming together of this idea that we can culture bacteria. We can sequence their genomes and we can. We can mess with genes, right genes in ways that we can turn them on that really allows you to untapped this reservoir that’s been tapped or untapped.
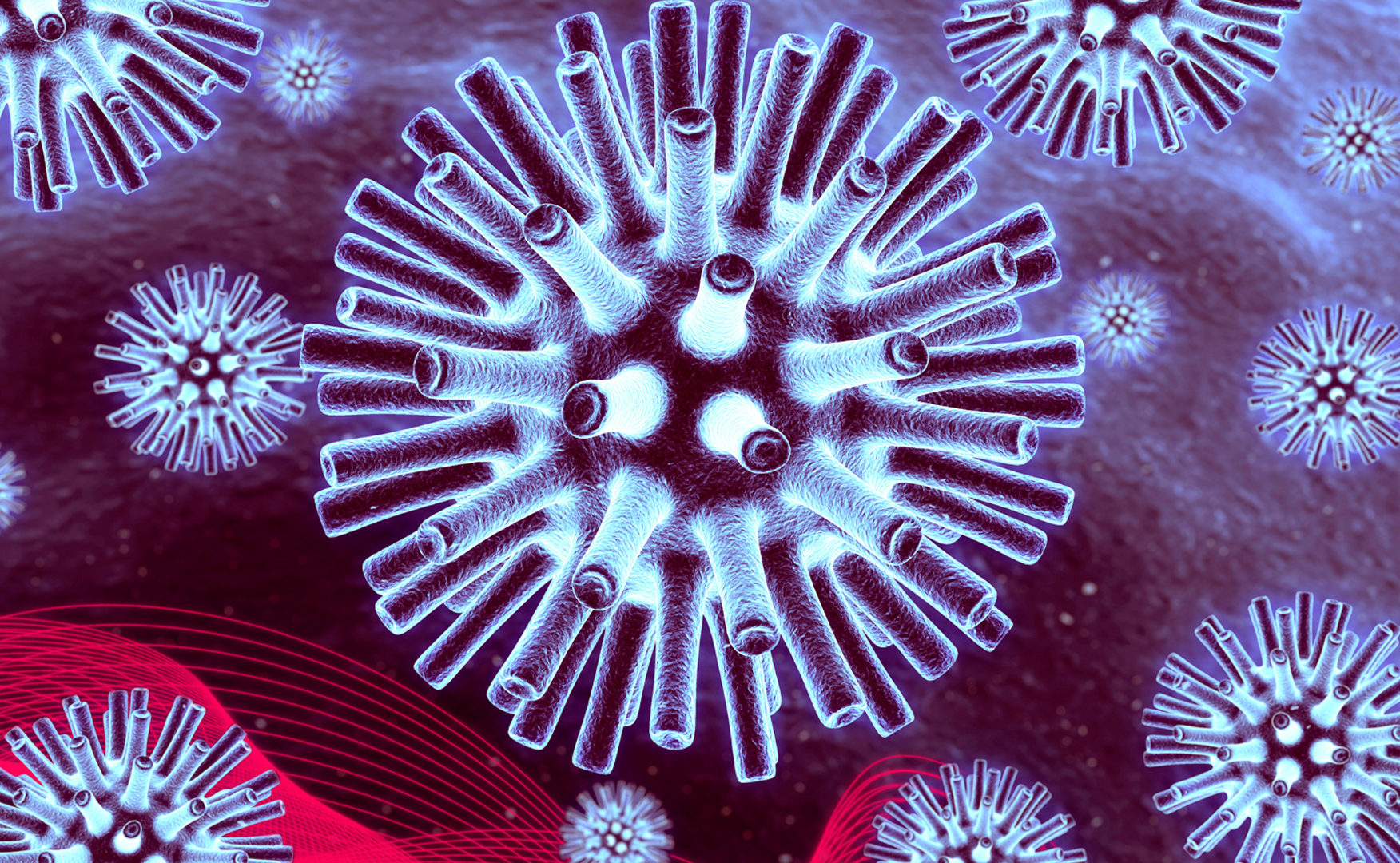
ZIMMER: So. So Vincent, I wanted to, to kind of shift gears here and look at a way of dealing with bacteria that’s totally doesn’t involve antibiotics at all. Um, there’s, and this is, this is kind of a long running idea of basically sending the enemies of bacteria against them. I mean, can you explain the idea of this kind of approach? What was sometimes called Phage therapy?
FISCHETTI: Well phage therapy actually started before antibiotic therapy. So, um, it was discovered by D’Herelle about 100 years ago. He discovered a, he had a vessel in the, it was cloudy with bacteria and suddenly it disappeared, just disappeared in his eyes. And he said some things in there that killed the bacteria, figured out that it was, it was a virus, a virus that only infected bacteria, bacteria phage, it’s called. And that started a revolution at the time to use phage to control infection. It was well before antibiotics.
ZIMMER: So these, so these viruses, they’re back, they’re known as bacteria phage. So what are we looking at? So the blue thing is bacteria.
FISCHETTI: The blue thing is the bacteria and the ring around that is the cell wall of bacteria. When it attaches, it injects its DNA into the cell and once that DNA gets into the cell, it takes over the self for the production, a new virus particles and once those virus particles are produced, the phage have a problem. They have to get out of that organism and they solve the problem by producing an enzyme called the lysine that drills a hole in the cell wall. And since the pressure inside the bacteria is greater than the external environment, the organism explodes and releases the bacteria phage that had been produced in the environment. And that’s phage therapy using those phage to kill the organism directly. What we’ve done is now taking that enzyme, the specific enzyme that drills a hole in the cell wall, we can produce it recombinantly, and when you add that enzyme externally, it does precisely what it did from the inside, drills a hole in the wall membrane externalizes and kills the organism, so we’ve developed the enzyme that the phage now uses to release its progeny phage. You could use phage themselves and that’s called phage therapy as a means to control bacteria, but you can use the enzyme to to accomplish the same thing.
ZIMMER: And there are particular species of phages that can go after particular species of bacteria?
FISCHETTI: The very specific, that’s the problem with phage therapy is that they’re highly specific for the organism that you’re going after. So in order to kill, for instance of Staph Aureus, you’ll need to produce a cocktail of maybe five or six or 10 or 15 phage to get around the chance of organisms becoming resistant because the bacteria become resistant very rapidly to phage.
ZIMMER: So they getting resistant to the phages as well. Antibiotics, they’re just evolving,
FISCHETTI: But that’s. That’s the normal system. The phage are trying to get into the organism, the bacteria trying to keep them out. So that balance has been going on for a billion years. Nobody wants to win that war, phage that want to win because if they win, all is gone. If the bacteria when. Well they can’t get enough DNA into them to to, to, to modulate their, their, their DNA themselves.
ZIMMER: Right. Because bacteria are taking in.
FISCHETTI: They are taking in DNA and so they need that. That acquisition of phage DNA that doesn’t kill them, that allows them to pick up genes if they, allows them to survive much more rapidly.
ZIMMER: So then there’s this molecule that phage make, this enzyme called lysine, and so you want to just try just using lysine rather than the whole virus.
FISCHETTI: We’ve been using lysine for almost 20 years now. We have lysine and the beauty of lysine is that they are very specific for the organism. We don’t see resistance, we’d never seen resistance. We’ve been doing this for 20 years that they cannot become resistant to lysines because they’d have to remodel their cell walls, so it would take them a very long time to become resistance. Probably hundreds of years before they become resistant to actual lysines.
FISCHETTI: So those are anthrax organisms and we’ve added lysine to them and you could see what happens to them. This is real time. They just explode and disappear. So you can take 10 billion organisms in a test tube and add up five few micrograms of lysine, within a couple of minutes, they’re gone, so it works quite well. We have enzymes and they’re quite specific, so you don’t run into the problem, the antibiotic problem where you kill everything. Your normal floor and the and the organism you’re trying to kill that. Quite the, the, the, the staff enzyme will kill staff. Anthrax enzyme kills anthrax. So you, you’re, you’re targeted killing. You’re not affecting your normal flora.
ZIMMER: So why isn’t everybody using lysine? I mean, what’s the, what are the challenges that you still face?
FISCHETTI: Well, we’re in clinical trials right now phase two. Phase one showed that it was quite safe. We’re in phase two in the hospital. So about 117 patients which would sure be done by the end of this year, treating MRSA infections, endocarditis, MRSA, septicemia and Endocarditis.
ZIMMER: Heart infections?
FISCHETTI: Heart valve infections and septicemia, bacteremia and we’ll know by the end of the year.
ZIMMER: So Janelle, I mean you had touched on this earlier about, you know, maybe paying more attention to our own sort of host health in terms of dealing with these infections and you know, you’re, you’ve been doing a lot of research into, into tolerance. Maybe you could sort of describe sort of the overall idea that you’re pursuing and then how do you know how that might translate into an actual treatment for a patient?
AYRES: Yeah. So I think that the, uh, what is evident to me with our perspective, uh, in developing antibiotics and antibiotic history and the approaches that have been described by my fellow panelists is that they’re all based on the question of how do we kill microbes and developing ways to kill microbes. And we are approaching this from a different perspective. We actually want to understand what it takes to enable a patient to return back to a healthy state and to survive infectious diseases. And um, there’s, we, I talked about sepsis and how in sepsis and this is the case with other infectious diseases as well, there’re significant physiological damage that occurs and that leads to physiological dysfunction. And in order for a patient to return to a healthy state and to survive an infection, they have to be able to. You have to be able to alleviate that damage that’s occurred, um, and, and restore the patient back to normal physiological function. And our assumption is that if we just kill the pathogen, we should be able to do that, but that’s not necessarily the case. You can have patients where antibiotics are effective in them, but the physiological damage that they’ve endured kills the patient anyways. And so there’s, we are taking a variety of approaches to understand, um, if our body encodes ways to protect us from infectious diseases by promoting health and alleviating physiological damage. And about 10 years ago now, we discovered that in addition to our immune system, which protects us from infections by killing pathogens, we’ve discovered that we encode a distinct defense strategy that we call the cooperative defense system. And this is a defense system that, um, is essential for us to survive infections. And it protects us by executing what we call tolerance mechanisms or disease tolerance mechanisms. And these are mechanisms that our bodies encode that alleviate physiological damage during microbial interactions.
AYRES: And so these are mechanisms that promote our health without killing the pathogen, so you can induce these, um, tolerance responses in, um, a host and they will be perfectly healthy and survive the infection despite having the pathogen present in their body. Um, and we like this approach because this provides a new avenue for treating infectious diseases that will enable us to promote survival of the patient, but they also, um, in theory should be what we call anti-evolution proof, meaning that pathogens should not evolve resistance to such strategies because we’re targeting the, the patient and the physiology that’s affected by the, um, the infectious disease without having a negative impact on microbial fitness.
ZIMMER: It almost sounds like the microbiome is so, so complex with hundreds or thousands of species that, how would you ever disentangle it well enough to be able to make it into medicine?
BLASER: You have to have a hypothesis. You have to conduct clinical trials. Clinical trials have advanced cancer therapy. They’ve converted HIV infection from a lethal disease to a completely treatable disease with longterm step-by-step clinical trials. That that’s what the field needs. Of course, that’s what we need in to to restore, to have working antibiotics, to develop new antibiotics as well.
ZIMMER: Yep. Sean.
BRADY: We do similar things with the human microbiome to do the soil because we look at the molecules that these bugs make and we’ve in fact found antibiotics that are effective against MRSA.
ZIMMER: So these are. These are antibiotics made in our bacteria living inside of us.
BRADY: Coded by the bacteria living inside of us.
ZIMMER: And we’re sort of antibiotics factories.
BLASER: Yeah, we, yeah. We may not need to undergraduates anymore. We may just have to mine our own microbiome.
HANDELSMAN: Or the undergraduates’.
FISCHETTI: To add to the complexity, we also have bacterial phage in our gut and they are modulating.
ZIMMER: So we have phages that are attacking our bacteria inside of us all the time.
FISCHETTI: We eat, drink phage all the time. Ten trillion phage pass through our gut into our tissues everyday, everyday. So they’re everywhere. There’s 10th of the 31 phage on earth, so they’re everywhere. We eat, drink phage all the time, so they’re in our gut, they’re modulating the organism up and down, so you have a bloom of phage and they are killing these particular organism. You have a reduction in up in that organism. We don’t know what physiological effects it has on our bodies, but it has to have an effect and, and understanding the modulation of phage and our gut flora is a, is another area that people are starting to look at.
ZIMMER: And then Janelle, like your own body is then responding to all these different things going on inside of you. I mean.
AYRES: Absolutely, it’s a bi-directional relationship. So, um, we’re, we’re recognizing the microorganisms that are in our intestine, but also some microbes induce host responses or immune responses to that are not effective against themselves, but will be effective against other microbes within the community. So, um, through this, bi-directional communication, it goes back to ecology 101. They’re, they’re using the host to also shape that ecosystem.
ZIMMER: So I’m gonna open it up to questions in a little bit. But before I do that, I just wanted to get a sense from all of you about sort of the human side of all of this. I mean, we, we talked about how the industry incentives are all quite perverse and you know, it takes time and effort to find these antibiotics or to develop these other alternatives. So are there, do you see changes in a good direction in terms of, of, you know, creating a sort of these scientific or social customs or, or, or procedures to help get us towards this better situation where you might use the, these things? Or are we just going to, you know, like not be able to define these replacements because there isn’t enough support for it. And Marty, what do you think?
BLASER: The bottom line is that we need to be better stewards of antibiotics. We could create 10 new antibiotics or 10 new lysines, but unless we use them better, uh, the, uh, the resistance will get to us. The bacteria are, are selected for resistance. So we’re, we have to reduce the variation in antibiotic use. They’re using antibiotics a lot less in Sweden than they are here. People are just as healthy as we are here. There’s a lot of regional variation in antibiotic use. There’s variation from doctor to doctor, the the practice, the public have to be better stewards. Understand that antibiotic use has cost. We’re using it as if it had no cost.
ZIMMER: So you think that we could even now, I mean not even talking about these amazing possibilities that we’ve just discussed, you think that we could reduce the amount of antibiotics that patients are taking and still be protecting.
BLASER: That will help us decrease the pressure. You know, one of the questions is why did C diff move out of the hospital into the community? Why did MRSA move from the hospital into the general community? But we might be able to get it back in.
ZIMMER: Right. So Janelle you were just nodding before. I mean, do you think.
AYRES: I think there’s some great data from antibiotic clinical trials from 1920s and 1930s where with certain trials, the, the group that received the placebo, 80 percent of them did just fine. We can clear infections on our own. We can survive infections on our own, um, and I think a lot of times by the time a patient shows up to the clinic to get the antibiotics, they, there are studies to suggest that they’ve already cleared the infection and now they’re just getting antibiotics because they have some residual symptoms from the infection. So I completely agree with Marty that if we can just temper our use of current, um, antibiotics that will help significantly.
ZIMMER: And what about you Sean? You were just talking about like, um, how much money an antibiotic might make and how much money is required to do it. So like how do you, how do you even, how do you get those thing numbers to balance out?
BRADY: I think the good thing is we’ve seen this tremendous effort in the past decade to try and solve the discovery problem. We still need more money there, but we clearly see there’s global impetus to say we need more antibiotics. Maybe there’re, I think there’re 50 recognized major efforts in the past decade to, to support antibiotic discovery internationally. So I see that going in the right direction. I really do. I don’t know that it’s going to happen fast enough, we’ll ever get enough money, but that’s in the right direction, but it’s the post antibiotic issue. Not only our use, but how do we market it? How do we, how do we let those things survive? I still think we have a lot of hard thinking to think about how we’re, how we’re going to do that and I don’t think we have, we have a solution. We have great examples we can go to. There are lots of things that countries do to put things in reserve. You can say our army is in reserve until we need it. Right? We pay a lot of money for that. Why not think of same models for antibiotics that we have them developed. They’re in reserve. We pay for them prior to their use, but before we need them. I mean there’s a lot of thought that has to go into that, but to me that’s where the gap is at the moment, but we need more money for, for, for development of antibiotics. We see money flooding in. We still need more, but there’s really still this question of how do we use them afterwards and how do we finance that worries me.
FISCHETTI: What might help is the fact that we’ve been using for years and decades or a broad spectrum antibiotics and they’re killing everything and the reasons for that is when you’re sick, you go to the hospital and the clinician needs to know what he’s going to treat you with. If he doesn’t know the bug that’s causing the infection he has to give you something that’s broad spectrum. If we had diagnostics at the bedside, so if someone comes into the hospital and we know exactly what organism’s causing the infection you can treat with an antibiotic that is specific for that organism. Would have very little effect on your normal flora, but we’re not at that point. We’re close. Our hospitals now can identify the organism fairly quickly.
ZIMMER: Fairly quickly meaning what kind of time scale?
FISCHETTI: Hours, so we’re at hours from days to hours. And if that. If you can do that, then you have antibiotics that are more channeled to the organism that you’re killing, which would cause less side effects. And I think that that might be a way to survive this type of issue that we’re having right now.
ZIMMER: And then what about sort of uh, these, um, less, we’ll call them less conventional things like phage therapy or using lysines or so. And do you like in terms of getting a regulatory approval for these things, do you do, do you think that that is able to move forward quickly enough or. Or are we, do we need a better way to sort of like take in new ideas and try to get them approved to be used?
FISCHETTI: Well, the lysine therapy has been quite successful in moving through the system. Phage therapy has an issue, because phage therapy is, is a concoction of many phage to control a particular infection. And since you could make a cocktail, I can make a different cocktail that causes the same infection. There is no IP so there’s no incentive. The develop phage therapy if it does work to some degree, but there’s no incentive there. But if you have a defined molecule then that, I think that the pathway to get it out out the door is quite good.
ZIMMER: Alright. So Jo, I’m just curious, are you, when you look ahead 50 years, do you see the sort of the dark picture they recast earlier or do you, are you optimistic? I mean what’s.
HANDELSMAN: I’m always the optimist, but I also have to be tempered by the fact that we developed a plan for antibiotic development and stewardship when I was in the White House and there were some really simple things in there that could have been done like stewardship of antibiotics in hospitals. So CDC has an eight point plan of what hospitals are supposed to do. We found that only 50 percent of hospitals in the United States followed that very, very simple plan, like having a strategy for an antibiotic use in the hospital, training personnel in antibiotics. It. It was really kind of depressing and appalling and we identified all the things mentioned here and then many others that we need to steward the antibiotics, use them less, have better diagnostics so that we know when to use them and we don’t even use the tools today that we have like diagnostics. I’ve, I’ve done this survey completely unscientific. I shouldn’t even talk about it, but it’s my little way of keeping tabs on the docks. I asked in my lab, when people go for a sore throat, go to the doctor, what do they do? And 10 years ago there was never a test. They just gave them the antibiotics in every case. And then slowly we started seeing the strep test, strep throat test being used. But even today, fewer than half are getting a test before they get antibiotics. That just seems irresponsible to me.
ZIMMER: Any guesses why? I mean Marty, what do you? I mean you’re the doctor? I mean why, what? I mean what, it doesn’t make sense.
BLASER: It’s the problem of transparency, the medical profession and the public overestimate the benefit of antibiotic and they underestimate the cost, the effects of antibiotics. And so, uh, we, we have, we have to fix that and I, I really agree about narrow spectrum antibiotics, you know, and, and as I said, antibiotics are falsely inexpensive, why, why give someone a $500 or $5,000 antibiotic when you can treat them with a $5 antibiotic. So the market’s broken, but we need to use tax money just like we need to use tax money to buy interstate highways, uh, that, that’s a public. Antibiotics are public good. We have to invest in, in, in antibiotics that will protect our future, uh, as, as a public good.
ZIMMER: Okay, um, we have microphones. A question right in the back there.
AUDIENCE: Thank you first off for the presentation, that was really useful. Um, I just have two quick questions. So first I’m being. So how advanced and what are the, what is the percentage accuracy on these diagnostic tools? Can they either be improved or is it just because these current antibiotics are cheaper, they’re just not getting that much visibility. And my second question is, are there currently government programs that are in place or in the pipeline? And the reason I ask this is because there’re orphan diseases out there that don’t have a large market either, but yet there are a lot of government programs that incentivize the innovations for this space. So I’m wondering if that’s something that’s happening in the pipeline right now that will encourage innovation in the space.
ZIMMER: Great. So let’s, uh, let’s, uh, let’s take these one at a time. So Vince maybe you could start us off in terms of the diagnostics. Is it just a case that we already have really good diagnosis but then they’re just not being used enough? Or are there a possibility to develop new kinds of technology to really get these things identified fast?
FISCHETTI: Well, right now they’re doing it by DNA analysis.
ZIMMER: So how does that work?
FISCHETTI: You just get a number of organisms, a few organisms from swab and they can take it and put it, extract the DNA, put it through a machine and identify certain genes certain pathogens have. And they can do that within hours. Sometimes they’d have to grow the organism very for only a few generations to get more organisms so they can extract more DNA. But it’s quite quite accurate. It just takes a little more time. It’s not at the bedside. It’s a few hours, but it’s better than what we used to have which was overnight. We’d have to culture it, let the grow, organisms grow overnight and then even another test usually two days before you get the identification.
ZIMMER: When you say at the bedside, are you saying, I mean like a doctor comes, a nurse comes and takes your temperature at the bedside, takes your blood pressure at the bedside or you’re saying-
FISCHETTI: Well like a rapid strep test is in a sense at the bedside. You can swab the throat and put it into a solution that digests the organism and they have an antibody that identifies a molecule on that organism. You can do that within 20 minutes. You get the results of that experiment. That’s at the bedside. We’re not there yet, but we’re close.
ZIMMER: And are hospitals like. It sounds from your, from your survey, I would guess that maybe hospitals are a little slow to really snap up the best of these diagnostics.
HANDELSMAN: They are used. Some are and some aren’t. Just like the simple practices to reduce antibiotic resistance, which don’t cost any money and in most cases some adopt them and some don’t.
ZIMMER: And Marty,
BLASER: I mean most antibiotics used in the United States and most countries are used in outpatients. They’re not used, so the focus, 90 percent of the antibiotics are used in outpatient, and most of the antibiotics are used for upper respiratory infections, which we know that a big fraction are viral and are not bacterial at all, so viral infections don’t respond to antibiotics. So we need a rapid diagnostic that will tell whether that outpatient walking in has a viral infection or bacterial infection.
ZIMMER: In the doctor’s office as well.
BLASER: If we had that tool, we could eliminate a lot of unnecessary antibiotic testing. One of the problems is that the antibiotic costs $5. The test might cost $500. So our health system isn’t, It’s not working.
ZIMMER: Okay. So after we get fix antibiotic problem, we’ll fix the healthcare system, right? Or first, what if, at the same time. Anyway, the second question was about what? What are, what are there? Are there any special government programs that are actually like trying to, to push research about resistance forward with what’s happening?
BLASER: So as, as you mentioned, I’m on this commission that Jo was involved in setting up called PACCARB, which is President Obama set it up by executive order and, and our mandate is to combat antibiotic resistant bacteria and we have five different areas, surveillance, stewardship, new diagnostics, therapeutics and international efforts working with other countries. So as, as part of these and, and the executive order, uh, money’s have gone into something called BARDA, which is to develop new antibiotics, to put money in, to make it more economically viable, to develop antibodies, to look at antibiotics like orphan diseases as well. They’re, they’re special stipulations that make it more attractive for companies to make products for orphan diseases.
ZIMMER: Great. Any more questions?
AUDIENCE: Is prevention still a big thing in terms of the washing of the hands thing, is that still the best thing we can do? I have one little version of that. I try not to touch anything when I go to the men’s room. Does that work?
BLASER: So soap and water works. There’s no question, but on the other hand, there are all these antibacterial products, uh, that are killing the good bacteria. Good bacteria help protect us against the bad bacteria against the invader. So are they doing more good or good? Doing more harm. And I don’t know either. These things have hardly been tested and the people who make them aren’t particularly interested in testing.
ZIMMER: So we should, we should just talk a little bit about. I mean, we’ve lot, I’ve been talking a lot about the gut, but the skin is covered in bacteria, right?
HANDELSMAN: And it’s a completely different flora than we have in our gut or our mouth or our ears. In fact, the two hands differ a left and right.
ZIMMER: So. And are they, are they, are they doing, are they doing good things for me right now?
HANDELSMAN: Yeah. They’re protecting your skin just like they protect any surface they’re on, they’re good guys. You have to get used to this respect for the microbes thing.
ZIMMER: Okay, okay, now I can handle this. And so, so if you use these sort of hand sanitizers with the antibacterials-
BLASER: There are times to use them in the hospital, it’s very important to use them because you have a lot of bad bacteria transmitting in hospitals. So washing the hands and a variety of different ways is important. And during flu season it’s very important because flu is transferred by people’s hands. But if you take all of that collectively, maybe that’s three percent of the time. The other 97 percent of the time, the benefit is just leaving our microbes alone.
HANDELSMAN: I think the biggest thing any of us can do is treat our flu symptoms very respectfully. Stay home, not, so you don’t transmit it, wash your hands with soap. Purell won’t help with flu, but uh, that much but certain, oh, well yeah, get get you saying get the shot. Get a vaccine. That’s right, and because I think more antibiotics are given for flu like symptoms that turn out to be viral, but we don’t have the test to prove that than probably any other disease, so I think if we kept the flu under control and that can be controlled just by behaviors and washing hands and breathing in people’s faces.
ZIMMER: When?
HANDELSMAN: Usually November or December till our early March events.
ZIMMER: Vince?
FISCHETTI: You have to realize that 90 percent of infections come in through the mucous membranes. They’re not coming in on your hands. They are coming in through mucus membranes. Your eyes, your your genital track. So when you touch something that’s contaminated, you’re not getting infected through your skin. It’s when you touch your nose, or you touch your mouth that the organism then gets it. That’s how it gets in.
AYRES: You have to have a wound. Your skin is a barrier.
FISCHETTI: The only other way is a wound. You’re bringing the organism from where the other, whatever you picked up and you touch your nose and how many times you touch your nose and your mouth.
HANDELSMAN: About 12 times an hour for the average person.
ZIMMER: Wow. In the back there.
AUDIENCE: I think multiple of you stadia, but you were basically because you were using bacteria. No, because you were developing and what do you got? Penicillin and all which came from soil bacteria and therefore the soil bacteria had natural built in resistance to the compound you were using. A question, is it possible to synthetically generate proteins or protein analogs which would bind to sites or would interfere in other ways with mechanisms for which things have not developed resistance to because they weren’t. They aren’t actually naturally occurring equivalent to penicillin.
ZIMMER: Yeah. That’s actually an interesting point is that I think they’ve done studies right where like they would look at old soil and actually actually find that there were some resistance, resistant microbes like before the invention of antibiotics.
HANDELSMAN: That’s right. They’re all over it. My, my group has studied a site in Alaska that’s essentially as pristine as you can find a site on earth and it has very little exposure to antibiotics and we find a large array of antibiotic resistance genes. We also have found that when, purely synthetic antibiotics had been introduced on the market, resistance has even faster in some cases than to the naturally occurring ones. Penicillin’s been on the market for what, 60 or more 70 years and it’s still useful. Some of the this synthetic antibiotics can’t even be used anymore because there’s so much resistance, so we’re dealing with evolution. I think that’s the answer to the question of why there’s no universal cure or prevention because we’re dealing with evolving organisms.
ZIMMER: So I guess the lesson is that bacteria are pretty awesome.
HANDELSMAN: They really are.
ZIMMER: All right. Well let’s give a hand for our panelists. Thank you for coming.
We have fallen woefully behind in the race to keep up with harmful bacteria as they continually evolve to outsmart our antibiotics, in fact, there are already superbugs we cannot defeat. Predictions are by 2050 there will be more deaths from infections than from cancer if we don’t solve this crisis. Join immunologists, biologists, and infectious disease specialists to explore some exciting new tools that may be our salvation in the battle against superbugs.
This program is part of the Big Ideas Series, made possible with support from the John Templeton Foundation.

Carl Zimmer is an award-winning columnist for the New York Times and the author of 13 books about science. His reporting has earned awards from the National Academies of Science, the American Association for the Advancement of Sciences, and the Online Journalism Association.
Read More
Janelle Ayres is an Associate Professor in the Nomis Center for Immunobiology and Microbial Pathogenesis at The Salk Institute for Biological Studies. Her pioneering research on host-pathogen interactions is redefining our definition of health.
Read More
Martin Blaser is the Singer Professor of Medicine, Professor of Microbiology, and Director of the Human Microbiome Program at NYU School of Medicine. He served as Chair, Department of Medicine from 2000-2012. A physician and microbiologist, Dr. Blaser studies the relationships we have with our persistently colonizing bacteria.
Read More
Vincent A. Fischetti Ph.D. is Professor and Head of the Laboratory of Bacterial Pathogenesis and Immunology at the Rockefeller University in New York. Fischetti’s research has focused on developing alternative methods to control bacterial infections.
Read More
Sean Brady graduated with a degree in molecular biology from Pomona College in Claremont, California and received his Ph.D. in organic chemistry from Cornell University. he later moved to Harvard Medical School as a fellow in the Institute of Chemistry and Cell Biology and was named an instructor in the department of biological chemistry and molecular pharmacology at Harvard Medical School.
Read More
Jo Handelsman is the Director of the Wisconsin Institute for Discovery at the University of Wisconsin-Madison, as well as a Vilas Research Professor and Howard Hughes Medical Institute Professor. She is responsible for groundbreaking studies in microbial communication and work in the field of metagenomics.
Read MoreCARL ZIMMER: Thank you all for coming. Tonight we’re going to talk about a very serious subject. Um, the situation that we face with antibiotic resistant bacteria. Antibiotics were once the silver bullet that seemed to be able to cure just about everything. Now we look at 23,000 antibiotic resistant bacterial infections every year. So let me introduce you to our panelists. Our first participant is the Director of the Wisconsin Institute for Discovery at the University of Wisconsin-Madison. She was a science advisor to President Barack Obama. Please welcome Jo Handelsman. Our next participant is a professor at Rockefeller University where he is head of the Laboratory of Bacterial Pathogenesis and Immunology. Please welcome Vincent Fischetti.
ZIMMER: Our next participant is an associate professor of Immunobiology and Microbial Pathogenesis at The Salk Institute. Please welcome Janelle Ayres.
ZIMMER: Our next participant is the Evnin Associate Professor at Rockefeller University. Please welcome Sean Brady.
ZIMMER: and finally the Singer Professor of Medicine in Microbiology, and the Director of the Human Microbiome Program at NYU School of Medicine. Please welcome Martin Blaser.
ZIMMER: Uh so, I thought that maybe a way to start would be to show a video. This was an experiment that was done at Harvard where basically scientists created at sort of gigantic petri dish, sort of kind of the size of an air hockey table basically, and they seeded it with bacteria on either side and then basically laced it with antibiotics. Starting at the edge with pretty mild levels and then as you go further in, it gets more and more deadly until the central band has a thousand times the lethal dose for Ecoli. It’s really kind of mind blowing. We’re going to see the bacteria, so just sort of hanging out there and now they’re multiplying. This is sort of time lapse, so when they hit that point, what they’re encountering that as antibiotics and then how are they getting past it? I mean you can see them.
JO HANDELSMAN: It takes a little bit of time and what they’re waiting for is growth of one or a very small number of cells in the population that are already resistant. And so although there were many, many billions of cells crossing the plate, probably one in a million would have resistance to the antibiotic, so once those started dividing and-
ZIMMER: So they’re dividing and one in a million just happens to gain this power to get past it?
HANDELSMAN: Well, they always had the power. It was preexisting in the population, but then when the whole population is, the rest of the population is stopped by the antibiotic because they’re inhibited by it. Then those few that are resistant start proliferating and then they take over and that’s exactly what it looks like in similar terms when it’s in the body, you know, you take an antibiotic and most of the bacteria will die, but there will be preexisting mutants in the population that are resistant.
ZIMMER: That’s great. Well not great, but it’s amazing.
HANDELSMAN: It is definitely not great.
ZIMMER: Yeah, no it didn’t. I know, I know. Don’t get me wrong. We think of antibiotics as, as the sort of heroic triumph of science. I mean, how did, how did we get to enjoy the benefits of antibiotics? I mean, how did that begin?
HANDELSMAN: Well, it started with a chance discovery from a by Sir Alexander Fleming. In the UK, who found a fungus on his plate that was clearly inhibiting growth of staphylococcus on, on the Petri dish, and he recognized what it was that this was a compound that was diffusing into the Auger and determined that it was what we now know of as penicillin, but it was many years before it can be used in any kind of broad scale way because he discovered that in 1929 and by the start of World War II, we still, we’re not using antibiotics and they weren’t in general use.
ZIMMER: Why not? I mean you, you discover a drug, you know, put it into practice. I mean, what was the holdup?
HANDELSMAN: They couldn’t make enough of it. That fungus produced some but not enough to go into large scale production. And so during the war a scientist named Ken Raper was worked for the USDA in Peoria and he decided as a war effort to put out the call for penicillin producing strains of penicillium mold. So he told everybody in Peoria to collect as many fruits and vegetables with that green blue fuzzy thing that you see on your bread and fruit to bring those to his lab. And people did and he had this large collection and it turned out it was his own technician who has gone down in history, as Moldy Mary now. Her name was actually Mary Hunt and she brought in the winning cantaloupe and it had a strain of penicillium mold that produces more penicillin than any other natural strain to this day. And so they started, they moved it right into commercial production and started pumping out large amounts of penicillin and they have enough to be able to ship it the penicillin to the troops in Europe. And so World War Two was the first war in which more people died directly of bullets and bombs than the infections that accompanied them.
ZIMMER: Wow. So, and then once, once the war is over, then antibiotic start to become more of just a general medicine for the public in general, right?
HANDELSMAN: Yeah. And at the same time there was interest in soil bacteria that produced antibiotics. And, and then after the war there was just this explosion of knowledge of people, culturing organisms from the soil, screening them for antibiotics and then moving into production. And so we had dozens of antibiotics coming onto the market in the next decades.
ZIMMER: Sean, I mean, how would you sort of describe like the sort of, the overall benefit of these discoveries of penicillin and some of these other early antibiotics? I mean, what I mean overall, like in terms of lives saved or someone, what are we looking at in terms of the scale of this?
BRADY: I think one of the figures that penicillin alone has saved 100 million lives.
ZIMMER: And that’s penicillin alone.
BRADY: Yeah. So if you think about that single picture that Joe talked to you, you see it in almost any microbiology textbook. That image has probably saved more lives than anything in the history of science. So you want one kind of thing in your office, you should hang that picture as a scientist because it’s made a larger impact on human health than anything but, but that, that whole discovery, even today we’re still using those antibiotics. So. So that’s the initial discovery, then you think about almost everything that came out of what we call the golden age of antibiotics, the forties, fifties, and sixties.
ZIMMER: So people were finding things not just on cantaloupe but in other-
BRADY: They are culturing soil bacteria largely and finding antibiotics. Almost every class of antibiotics that we use today was discovered in that that time period. We have relied on antibiotic defense really of those molecules and continually using versions of those molecules up until today. And that’s why we’re in the position we are today. We, we’ve largely ceased discovering antibiotics after the golden age, the late sixties, early seventies. Because we thought we were done. We thought we had solutions to these problems. That’s how good those initial discoveries were. How, how much of an impact they made on human health.
ZIMMER: What’s your sense of like when it started to become clear that things weren’t going so well? Like when? When do you think that the sort of scientific medical community said, I think we have a problem?
BLASER: Well that happened pretty quickly. I mean we were seeing resistant organisms to penicillin early on. It was, it started
ZIMMER: Like a matter of a few years after?
BLASER: Probably a year or two
ZIMMER: After the introduction of penicillin.
BLASER: Exactly we already started to see early stages of resistance, but you know, was it an organism here, an organism there, but, but it was occurring at that time and it’s been occurring at an accelerated rate since then.
ZIMMER: Right. So Marty, what do you think is, what would you say would be like one of the main factors that explain sort of how we got to this point in terms of resistance? Like what are we doing that is causing all of these bacteria now to be just so dangerous?
BLASER: So, uh, the short answer is that Darwin was right and that is that there is survival of the fittest. It’s selection. We are using antibiotics in such magnitude because of the miraculous nature of antibiotics, both the public and the profession says, well, why don’t we just treat this person with antibiotics even if their symptoms are minimal. So there’s enormous pressure, selective pressure of antibiotic use and it’s just, it’s just a mathematical certainty that there’ll be resistance, but it’s not linear. It’s, it’s geometric because of the properties of bacteria growing.
FISCHETTI: Yes, but you have to remember that bacteria come, most of them come from the soil and antibiotics are in the soil, so they’ve learned for millions of years how to deal with antibiotics. So the systems are there for as long as you. If you expose them to antibiotics, those systems become heightened, then become resistant. So they, they’ve seen these drugs or similar drugs or antibiotics type molecules for hundreds and hundreds of thousands, millions of years.
ZIMMER: Marty, you, you’ve also been talking a lot and writing a lot about the fact that our antibiotics are not precision weapons that you know, you use them against Ecoli, MRSA, and so on, but that’s not the only thing that’s going to affect.
BLASER: Yeah, so so antibiotics came of age when we were, when we were really trying to eliminate these bad pathogens, but no one really considered what was the effect of the antibiotics or the normal bacteria living in the body, the normal bacteria that we call the microbiome, but now it’s clear that that when you take an antibiotic for a skin infection or lung or urinary tract infection, that antibiotic is getting everywhere in the body and it is selecting for resistant organisms in that body. That’s suppressing some organisms and other organisms are coming up and maybe some organisms are becoming extinct as well.
ZIMMER: So these are organisms that we might actually depend on. It might be actually beneficial for us.
BLASER: And so in fact we know that one of the main defenses against infection are our residual. Our normal organisms there, there, there, the coast guard, they are protecting against invaders. They don’t want to share their turf and 50 years ago it was shown that if you pretreat mice or other laboratory animals with antibiotics and then give them a pathogen like Salmonella, the, the level of Salmonella that it takes to kill the mouse goes down by four logs, you know, by 10,000 falls.
ZIMMER: So Sean, I mean someone might say like, well we have all these gigantic pharmaceutical companies. There’s lots of money that they can throw at the problem. You know, there was penicillin and then there were other things I can think of mycin and you know, you know, science marches on. So we’ve got like more in the pipeline, right?
BRADY: That’s the unfortunate thing. We have almost nothing in the pipeline.
ZIMMER: Almost nothing.
BRADY: You can, you can ascribe that to a number of different reasons. We don’t get in a crisis because of one thing, but we get in it because many things came together that we probably didn’t foresee. One of them being that our first round of antibiotics worked so well right? That golden age of antibiotics when we were describing them, people thought we were done and so so over the next ensuing 30 years antibody discovery programs, both in academic and industrial settings largely shut down and so there are almost no pharmaceutical industries that are putting at least the effort they used to put in to finding antibiotics. The second thing is then if we’d been using antibiotics, the same ones for 30 years, that means they don’t cost us anything anymore. They’re all generics. You can get an antibiotic for somewhere between free and twenty cents a day in many parts of the world, so now you have an infrastructure that doesn’t exist and you have a financial structure that doesn’t support the development of antibiotics. So we are at a certain point trying to figure out how to restart that pharmaceutical industry and how to make it worthwhile to restart it. Have to be some major things changed.
HANDELSMAN: It’s in direct competition with chronic disease which is much more lucrative for the companies because it drug you take for the rest of your life is obviously going to make them more money than a drug you take for five days and then stop, and so even even now with the crisis that we all know we’re in, very few companies want to move back into that area.
FISCHETTI: And what they’re doing is taking a drug that worked, became, an organism, becomes resistant, and they just make a modification on that drug. It’s cheaper for them to do that than to start from the beginning and now the virus can become resistant much more rapidly. So they work for maybe a year or two and then they can’t use them anymore.
ZIMMER: Marty.
BLASER: And then there’s yet another problem and that is that bacteria don’t respect borders and so what that means is that if, if a resistant organism arises in another country like India or China, it doesn’t take too long for it to come over here and because antibiotics are so inexpensive and because people think that they’re so miraculous. In many of these countries, people are able to get antibiotics over the counter, no prescription necessary. Parents are giving their kids 10 courses of antibiotics a year in, in some recent studies funded by the Gates Foundation, tremendous antibiotic pressure, very low cost, but somebody’s making money on those antibiotics. Resistant organisms are arising and then there are the crossing all over the world,
ZIMMER: So this, so this sort of cheap marketplace of antibiotics over the counter and so on is even helping to drive on-
BLASER: The whole antibiotic market is broken. Antibiotics are in one sense too cheap and and, and are therefore overused and abused. And on the other hand there’s no incentive to create new antibiotics that we want to keep and put in reserve for important infections, which won’t affect tens of millions of people so that there isn’t that market. So the market, the economic model for antibiotics is just broken.
BRADY: Just, just to put a number on that, right? Yeah. So the most recent, they’re going to differ a little bit, but let’s say the six months, recent antibiotics that came to market made about $10,000,000 each last year. 10, 10 million each. Right? Okay, that seems like a lot of money, but just let’s say you’ve done all the clinical trials you need and now you need to synthesize a production scale an antibiotic. It’s $150,000,000 investment, right? And the reason these things make a little money is, is you don’t want to use them. You don’t want to use in this frontline defense, right? You want to put them in reserve until you absolutely need them. And so where’s the incentive? If, if forget the hundreds of millions you put into development, just to make the thing costs you 10 times which you can sell it for, sell it for a year. We really have to rethink how we, how we market these things, how we as a community decide we’re going to put antibiotics in reserve and put an upfront and of realization that these things are there. We need to pay for them as a community because we’re going to need them some day.
ZIMMER: Alright, so let’s, let’s brighten things up a bit by like actually, you know, you folks are actually working on things. So maybe we’ll start. We’ll start with antibiotics themselves, with new antibiotics. So with Jo and Sean’s work. So, so, so you’ve been going back to the soil, the soil that brought us all these original drugs. You think you think there are more there for us to find?
HANDELSMAN: I do. I’m so, for a long time I went to other methods for antibiotic discovery and you’ll hear about some of those that Sean’s developed soon, but the reason I did that was that there were some references from the nineties that said that the soil was mined. It was fully tapped and I’ve gone back to the data and I can’t find the data and so now I question whether that’s really true because in the ensuing decades my lab just spontaneously discovered antibiotics, novel antibiotics from soil that hadn’t been discovered and we weren’t even looking in some cases. And so I. It just occurred to me one day, wait a minute, it’s not mined if we’re finding them and so that’s the approach we’re taking is going back and asking what is the frequency of new compounds? There was one paper that said the rediscovery rate would be 99 percent, so if you found 100 compounds, 99 of them would be already known. Well that’s actually not so bad if it’s true because we can look at a lot more than 100 compounds with today’s methods, but. But I’m not even sure that that’s true because it wasn’t really based on at least published data. Maybe somebody in a pharmaceutical company has the data, but we haven’t seen it.
ZIMMER: So are there particular places that you like to go look for new antibiotics? In a particular soil that is you like or is it just in your backyard?
HANDELSMAN: Well, we’re looking at across the world, so we have a worldwide network of undergraduate students. Undergraduates who are a fantastic and very creative workforce. So we developed a course that is known as the Small World Initiative and it’s taught in 15 countries and all over the United States and about 10,000 students a year take the course and they dig up soil from whatever environment is interesting to them and they come up with more interesting reasons than I ever would for why an environment is interesting. And and so they have this great variety of soils. They’re isolating very interesting antibiotic producing organisms and now we have to go into the next stage which is figuring out what antibiotics are produced. So we think that if we have 10,000 students, each one gets at least 10 antibiotic producing organisms per year. That’s a lot of candidates. And so if we can crank through enough of them, even if that one percent rediscovery or 99 percent rediscovery rate is correct, we still have a lot of new compounds to look at.
ZIMMER: So Sean, what kind of approach are you taking to searching for these, these new antibiotics?
BRADY: So about 20 years ago now, I guess, Jo and a few other people were thinking along these ideas, thinking about is there a reservoir in soil still of, of natural products and, and the thing that that percolated to the top of the thinking of these people was that there’s data from even longer ago, maybe 120 years ago that it appears we don’t culture most of the bacteria out of the environment, that actually the bugs we’ve been playing with represent a small fraction of the bacteria in the environment.
ZIMMER: So let me ask you, so if you like take a sample of a little sample of soil, first of all, like how many microbes are in there and how much DNA are you talking about that you’re looking at from all of them?
BRADY: So it depends on whose numbers, let’s say is there’s thousands, maybe 10,000 different microbes of which we culture about one percent.
ZIMMER: Just one percent,.
BRADY: Just one percent. And again, people have done better nowadays, but they don’t solve the other problem, which is even if we can culture bacteria, we don’t turn on their genes. Right? So even if you can bring bacteria in the lab, they don’t know how to turn on the genes, they’re gonna make antibiotics for us. And so, so what we want to do is just look at their DNA and you can get huge amounts of DNA at least in the context of molecular biology out of a single gram of soil.
BRADY: And so it’s the coming together of this idea that we can culture bacteria. We can sequence their genomes and we can. We can mess with genes, right genes in ways that we can turn them on that really allows you to untapped this reservoir that’s been tapped or untapped.
ZIMMER: So. So Vincent, I wanted to, to kind of shift gears here and look at a way of dealing with bacteria that’s totally doesn’t involve antibiotics at all. Um, there’s, and this is, this is kind of a long running idea of basically sending the enemies of bacteria against them. I mean, can you explain the idea of this kind of approach? What was sometimes called Phage therapy?
FISCHETTI: Well phage therapy actually started before antibiotic therapy. So, um, it was discovered by D’Herelle about 100 years ago. He discovered a, he had a vessel in the, it was cloudy with bacteria and suddenly it disappeared, just disappeared in his eyes. And he said some things in there that killed the bacteria, figured out that it was, it was a virus, a virus that only infected bacteria, bacteria phage, it’s called. And that started a revolution at the time to use phage to control infection. It was well before antibiotics.
ZIMMER: So these, so these viruses, they’re back, they’re known as bacteria phage. So what are we looking at? So the blue thing is bacteria.
FISCHETTI: The blue thing is the bacteria and the ring around that is the cell wall of bacteria. When it attaches, it injects its DNA into the cell and once that DNA gets into the cell, it takes over the self for the production, a new virus particles and once those virus particles are produced, the phage have a problem. They have to get out of that organism and they solve the problem by producing an enzyme called the lysine that drills a hole in the cell wall. And since the pressure inside the bacteria is greater than the external environment, the organism explodes and releases the bacteria phage that had been produced in the environment. And that’s phage therapy using those phage to kill the organism directly. What we’ve done is now taking that enzyme, the specific enzyme that drills a hole in the cell wall, we can produce it recombinantly, and when you add that enzyme externally, it does precisely what it did from the inside, drills a hole in the wall membrane externalizes and kills the organism, so we’ve developed the enzyme that the phage now uses to release its progeny phage. You could use phage themselves and that’s called phage therapy as a means to control bacteria, but you can use the enzyme to to accomplish the same thing.
ZIMMER: And there are particular species of phages that can go after particular species of bacteria?
FISCHETTI: The very specific, that’s the problem with phage therapy is that they’re highly specific for the organism that you’re going after. So in order to kill, for instance of Staph Aureus, you’ll need to produce a cocktail of maybe five or six or 10 or 15 phage to get around the chance of organisms becoming resistant because the bacteria become resistant very rapidly to phage.
ZIMMER: So they getting resistant to the phages as well. Antibiotics, they’re just evolving,
FISCHETTI: But that’s. That’s the normal system. The phage are trying to get into the organism, the bacteria trying to keep them out. So that balance has been going on for a billion years. Nobody wants to win that war, phage that want to win because if they win, all is gone. If the bacteria when. Well they can’t get enough DNA into them to to, to, to modulate their, their, their DNA themselves.
ZIMMER: Right. Because bacteria are taking in.
FISCHETTI: They are taking in DNA and so they need that. That acquisition of phage DNA that doesn’t kill them, that allows them to pick up genes if they, allows them to survive much more rapidly.
ZIMMER: So then there’s this molecule that phage make, this enzyme called lysine, and so you want to just try just using lysine rather than the whole virus.
FISCHETTI: We’ve been using lysine for almost 20 years now. We have lysine and the beauty of lysine is that they are very specific for the organism. We don’t see resistance, we’d never seen resistance. We’ve been doing this for 20 years that they cannot become resistant to lysines because they’d have to remodel their cell walls, so it would take them a very long time to become resistance. Probably hundreds of years before they become resistant to actual lysines.
FISCHETTI: So those are anthrax organisms and we’ve added lysine to them and you could see what happens to them. This is real time. They just explode and disappear. So you can take 10 billion organisms in a test tube and add up five few micrograms of lysine, within a couple of minutes, they’re gone, so it works quite well. We have enzymes and they’re quite specific, so you don’t run into the problem, the antibiotic problem where you kill everything. Your normal floor and the and the organism you’re trying to kill that. Quite the, the, the, the staff enzyme will kill staff. Anthrax enzyme kills anthrax. So you, you’re, you’re targeted killing. You’re not affecting your normal flora.
ZIMMER: So why isn’t everybody using lysine? I mean, what’s the, what are the challenges that you still face?
FISCHETTI: Well, we’re in clinical trials right now phase two. Phase one showed that it was quite safe. We’re in phase two in the hospital. So about 117 patients which would sure be done by the end of this year, treating MRSA infections, endocarditis, MRSA, septicemia and Endocarditis.
ZIMMER: Heart infections?
FISCHETTI: Heart valve infections and septicemia, bacteremia and we’ll know by the end of the year.
ZIMMER: So Janelle, I mean you had touched on this earlier about, you know, maybe paying more attention to our own sort of host health in terms of dealing with these infections and you know, you’re, you’ve been doing a lot of research into, into tolerance. Maybe you could sort of describe sort of the overall idea that you’re pursuing and then how do you know how that might translate into an actual treatment for a patient?
AYRES: Yeah. So I think that the, uh, what is evident to me with our perspective, uh, in developing antibiotics and antibiotic history and the approaches that have been described by my fellow panelists is that they’re all based on the question of how do we kill microbes and developing ways to kill microbes. And we are approaching this from a different perspective. We actually want to understand what it takes to enable a patient to return back to a healthy state and to survive infectious diseases. And um, there’s, we, I talked about sepsis and how in sepsis and this is the case with other infectious diseases as well, there’re significant physiological damage that occurs and that leads to physiological dysfunction. And in order for a patient to return to a healthy state and to survive an infection, they have to be able to. You have to be able to alleviate that damage that’s occurred, um, and, and restore the patient back to normal physiological function. And our assumption is that if we just kill the pathogen, we should be able to do that, but that’s not necessarily the case. You can have patients where antibiotics are effective in them, but the physiological damage that they’ve endured kills the patient anyways. And so there’s, we are taking a variety of approaches to understand, um, if our body encodes ways to protect us from infectious diseases by promoting health and alleviating physiological damage. And about 10 years ago now, we discovered that in addition to our immune system, which protects us from infections by killing pathogens, we’ve discovered that we encode a distinct defense strategy that we call the cooperative defense system. And this is a defense system that, um, is essential for us to survive infections. And it protects us by executing what we call tolerance mechanisms or disease tolerance mechanisms. And these are mechanisms that our bodies encode that alleviate physiological damage during microbial interactions.
AYRES: And so these are mechanisms that promote our health without killing the pathogen, so you can induce these, um, tolerance responses in, um, a host and they will be perfectly healthy and survive the infection despite having the pathogen present in their body. Um, and we like this approach because this provides a new avenue for treating infectious diseases that will enable us to promote survival of the patient, but they also, um, in theory should be what we call anti-evolution proof, meaning that pathogens should not evolve resistance to such strategies because we’re targeting the, the patient and the physiology that’s affected by the, um, the infectious disease without having a negative impact on microbial fitness.
ZIMMER: It almost sounds like the microbiome is so, so complex with hundreds or thousands of species that, how would you ever disentangle it well enough to be able to make it into medicine?
BLASER: You have to have a hypothesis. You have to conduct clinical trials. Clinical trials have advanced cancer therapy. They’ve converted HIV infection from a lethal disease to a completely treatable disease with longterm step-by-step clinical trials. That that’s what the field needs. Of course, that’s what we need in to to restore, to have working antibiotics, to develop new antibiotics as well.
ZIMMER: Yep. Sean.
BRADY: We do similar things with the human microbiome to do the soil because we look at the molecules that these bugs make and we’ve in fact found antibiotics that are effective against MRSA.
ZIMMER: So these are. These are antibiotics made in our bacteria living inside of us.
BRADY: Coded by the bacteria living inside of us.
ZIMMER: And we’re sort of antibiotics factories.
BLASER: Yeah, we, yeah. We may not need to undergraduates anymore. We may just have to mine our own microbiome.
HANDELSMAN: Or the undergraduates’.
FISCHETTI: To add to the complexity, we also have bacterial phage in our gut and they are modulating.
ZIMMER: So we have phages that are attacking our bacteria inside of us all the time.
FISCHETTI: We eat, drink phage all the time. Ten trillion phage pass through our gut into our tissues everyday, everyday. So they’re everywhere. There’s 10th of the 31 phage on earth, so they’re everywhere. We eat, drink phage all the time, so they’re in our gut, they’re modulating the organism up and down, so you have a bloom of phage and they are killing these particular organism. You have a reduction in up in that organism. We don’t know what physiological effects it has on our bodies, but it has to have an effect and, and understanding the modulation of phage and our gut flora is a, is another area that people are starting to look at.
ZIMMER: And then Janelle, like your own body is then responding to all these different things going on inside of you. I mean.
AYRES: Absolutely, it’s a bi-directional relationship. So, um, we’re, we’re recognizing the microorganisms that are in our intestine, but also some microbes induce host responses or immune responses to that are not effective against themselves, but will be effective against other microbes within the community. So, um, through this, bi-directional communication, it goes back to ecology 101. They’re, they’re using the host to also shape that ecosystem.
ZIMMER: So I’m gonna open it up to questions in a little bit. But before I do that, I just wanted to get a sense from all of you about sort of the human side of all of this. I mean, we, we talked about how the industry incentives are all quite perverse and you know, it takes time and effort to find these antibiotics or to develop these other alternatives. So are there, do you see changes in a good direction in terms of, of, you know, creating a sort of these scientific or social customs or, or, or procedures to help get us towards this better situation where you might use the, these things? Or are we just going to, you know, like not be able to define these replacements because there isn’t enough support for it. And Marty, what do you think?
BLASER: The bottom line is that we need to be better stewards of antibiotics. We could create 10 new antibiotics or 10 new lysines, but unless we use them better, uh, the, uh, the resistance will get to us. The bacteria are, are selected for resistance. So we’re, we have to reduce the variation in antibiotic use. They’re using antibiotics a lot less in Sweden than they are here. People are just as healthy as we are here. There’s a lot of regional variation in antibiotic use. There’s variation from doctor to doctor, the the practice, the public have to be better stewards. Understand that antibiotic use has cost. We’re using it as if it had no cost.
ZIMMER: So you think that we could even now, I mean not even talking about these amazing possibilities that we’ve just discussed, you think that we could reduce the amount of antibiotics that patients are taking and still be protecting.
BLASER: That will help us decrease the pressure. You know, one of the questions is why did C diff move out of the hospital into the community? Why did MRSA move from the hospital into the general community? But we might be able to get it back in.
ZIMMER: Right. So Janelle you were just nodding before. I mean, do you think.
AYRES: I think there’s some great data from antibiotic clinical trials from 1920s and 1930s where with certain trials, the, the group that received the placebo, 80 percent of them did just fine. We can clear infections on our own. We can survive infections on our own, um, and I think a lot of times by the time a patient shows up to the clinic to get the antibiotics, they, there are studies to suggest that they’ve already cleared the infection and now they’re just getting antibiotics because they have some residual symptoms from the infection. So I completely agree with Marty that if we can just temper our use of current, um, antibiotics that will help significantly.
ZIMMER: And what about you Sean? You were just talking about like, um, how much money an antibiotic might make and how much money is required to do it. So like how do you, how do you even, how do you get those thing numbers to balance out?
BRADY: I think the good thing is we’ve seen this tremendous effort in the past decade to try and solve the discovery problem. We still need more money there, but we clearly see there’s global impetus to say we need more antibiotics. Maybe there’re, I think there’re 50 recognized major efforts in the past decade to, to support antibiotic discovery internationally. So I see that going in the right direction. I really do. I don’t know that it’s going to happen fast enough, we’ll ever get enough money, but that’s in the right direction, but it’s the post antibiotic issue. Not only our use, but how do we market it? How do we, how do we let those things survive? I still think we have a lot of hard thinking to think about how we’re, how we’re going to do that and I don’t think we have, we have a solution. We have great examples we can go to. There are lots of things that countries do to put things in reserve. You can say our army is in reserve until we need it. Right? We pay a lot of money for that. Why not think of same models for antibiotics that we have them developed. They’re in reserve. We pay for them prior to their use, but before we need them. I mean there’s a lot of thought that has to go into that, but to me that’s where the gap is at the moment, but we need more money for, for, for development of antibiotics. We see money flooding in. We still need more, but there’s really still this question of how do we use them afterwards and how do we finance that worries me.
FISCHETTI: What might help is the fact that we’ve been using for years and decades or a broad spectrum antibiotics and they’re killing everything and the reasons for that is when you’re sick, you go to the hospital and the clinician needs to know what he’s going to treat you with. If he doesn’t know the bug that’s causing the infection he has to give you something that’s broad spectrum. If we had diagnostics at the bedside, so if someone comes into the hospital and we know exactly what organism’s causing the infection you can treat with an antibiotic that is specific for that organism. Would have very little effect on your normal flora, but we’re not at that point. We’re close. Our hospitals now can identify the organism fairly quickly.
ZIMMER: Fairly quickly meaning what kind of time scale?
FISCHETTI: Hours, so we’re at hours from days to hours. And if that. If you can do that, then you have antibiotics that are more channeled to the organism that you’re killing, which would cause less side effects. And I think that that might be a way to survive this type of issue that we’re having right now.
ZIMMER: And then what about sort of uh, these, um, less, we’ll call them less conventional things like phage therapy or using lysines or so. And do you like in terms of getting a regulatory approval for these things, do you do, do you think that that is able to move forward quickly enough or. Or are we, do we need a better way to sort of like take in new ideas and try to get them approved to be used?
FISCHETTI: Well, the lysine therapy has been quite successful in moving through the system. Phage therapy has an issue, because phage therapy is, is a concoction of many phage to control a particular infection. And since you could make a cocktail, I can make a different cocktail that causes the same infection. There is no IP so there’s no incentive. The develop phage therapy if it does work to some degree, but there’s no incentive there. But if you have a defined molecule then that, I think that the pathway to get it out out the door is quite good.
ZIMMER: Alright. So Jo, I’m just curious, are you, when you look ahead 50 years, do you see the sort of the dark picture they recast earlier or do you, are you optimistic? I mean what’s.
HANDELSMAN: I’m always the optimist, but I also have to be tempered by the fact that we developed a plan for antibiotic development and stewardship when I was in the White House and there were some really simple things in there that could have been done like stewardship of antibiotics in hospitals. So CDC has an eight point plan of what hospitals are supposed to do. We found that only 50 percent of hospitals in the United States followed that very, very simple plan, like having a strategy for an antibiotic use in the hospital, training personnel in antibiotics. It. It was really kind of depressing and appalling and we identified all the things mentioned here and then many others that we need to steward the antibiotics, use them less, have better diagnostics so that we know when to use them and we don’t even use the tools today that we have like diagnostics. I’ve, I’ve done this survey completely unscientific. I shouldn’t even talk about it, but it’s my little way of keeping tabs on the docks. I asked in my lab, when people go for a sore throat, go to the doctor, what do they do? And 10 years ago there was never a test. They just gave them the antibiotics in every case. And then slowly we started seeing the strep test, strep throat test being used. But even today, fewer than half are getting a test before they get antibiotics. That just seems irresponsible to me.
ZIMMER: Any guesses why? I mean Marty, what do you? I mean you’re the doctor? I mean why, what? I mean what, it doesn’t make sense.
BLASER: It’s the problem of transparency, the medical profession and the public overestimate the benefit of antibiotic and they underestimate the cost, the effects of antibiotics. And so, uh, we, we have, we have to fix that and I, I really agree about narrow spectrum antibiotics, you know, and, and as I said, antibiotics are falsely inexpensive, why, why give someone a $500 or $5,000 antibiotic when you can treat them with a $5 antibiotic. So the market’s broken, but we need to use tax money just like we need to use tax money to buy interstate highways, uh, that, that’s a public. Antibiotics are public good. We have to invest in, in, in antibiotics that will protect our future, uh, as, as a public good.
ZIMMER: Okay, um, we have microphones. A question right in the back there.
AUDIENCE: Thank you first off for the presentation, that was really useful. Um, I just have two quick questions. So first I’m being. So how advanced and what are the, what is the percentage accuracy on these diagnostic tools? Can they either be improved or is it just because these current antibiotics are cheaper, they’re just not getting that much visibility. And my second question is, are there currently government programs that are in place or in the pipeline? And the reason I ask this is because there’re orphan diseases out there that don’t have a large market either, but yet there are a lot of government programs that incentivize the innovations for this space. So I’m wondering if that’s something that’s happening in the pipeline right now that will encourage innovation in the space.
ZIMMER: Great. So let’s, uh, let’s, uh, let’s take these one at a time. So Vince maybe you could start us off in terms of the diagnostics. Is it just a case that we already have really good diagnosis but then they’re just not being used enough? Or are there a possibility to develop new kinds of technology to really get these things identified fast?
FISCHETTI: Well, right now they’re doing it by DNA analysis.
ZIMMER: So how does that work?
FISCHETTI: You just get a number of organisms, a few organisms from swab and they can take it and put it, extract the DNA, put it through a machine and identify certain genes certain pathogens have. And they can do that within hours. Sometimes they’d have to grow the organism very for only a few generations to get more organisms so they can extract more DNA. But it’s quite quite accurate. It just takes a little more time. It’s not at the bedside. It’s a few hours, but it’s better than what we used to have which was overnight. We’d have to culture it, let the grow, organisms grow overnight and then even another test usually two days before you get the identification.
ZIMMER: When you say at the bedside, are you saying, I mean like a doctor comes, a nurse comes and takes your temperature at the bedside, takes your blood pressure at the bedside or you’re saying-
FISCHETTI: Well like a rapid strep test is in a sense at the bedside. You can swab the throat and put it into a solution that digests the organism and they have an antibody that identifies a molecule on that organism. You can do that within 20 minutes. You get the results of that experiment. That’s at the bedside. We’re not there yet, but we’re close.
ZIMMER: And are hospitals like. It sounds from your, from your survey, I would guess that maybe hospitals are a little slow to really snap up the best of these diagnostics.
HANDELSMAN: They are used. Some are and some aren’t. Just like the simple practices to reduce antibiotic resistance, which don’t cost any money and in most cases some adopt them and some don’t.
ZIMMER: And Marty,
BLASER: I mean most antibiotics used in the United States and most countries are used in outpatients. They’re not used, so the focus, 90 percent of the antibiotics are used in outpatient, and most of the antibiotics are used for upper respiratory infections, which we know that a big fraction are viral and are not bacterial at all, so viral infections don’t respond to antibiotics. So we need a rapid diagnostic that will tell whether that outpatient walking in has a viral infection or bacterial infection.
ZIMMER: In the doctor’s office as well.
BLASER: If we had that tool, we could eliminate a lot of unnecessary antibiotic testing. One of the problems is that the antibiotic costs $5. The test might cost $500. So our health system isn’t, It’s not working.
ZIMMER: Okay. So after we get fix antibiotic problem, we’ll fix the healthcare system, right? Or first, what if, at the same time. Anyway, the second question was about what? What are, what are there? Are there any special government programs that are actually like trying to, to push research about resistance forward with what’s happening?
BLASER: So as, as you mentioned, I’m on this commission that Jo was involved in setting up called PACCARB, which is President Obama set it up by executive order and, and our mandate is to combat antibiotic resistant bacteria and we have five different areas, surveillance, stewardship, new diagnostics, therapeutics and international efforts working with other countries. So as, as part of these and, and the executive order, uh, money’s have gone into something called BARDA, which is to develop new antibiotics, to put money in, to make it more economically viable, to develop antibodies, to look at antibiotics like orphan diseases as well. They’re, they’re special stipulations that make it more attractive for companies to make products for orphan diseases.
ZIMMER: Great. Any more questions?
AUDIENCE: Is prevention still a big thing in terms of the washing of the hands thing, is that still the best thing we can do? I have one little version of that. I try not to touch anything when I go to the men’s room. Does that work?
BLASER: So soap and water works. There’s no question, but on the other hand, there are all these antibacterial products, uh, that are killing the good bacteria. Good bacteria help protect us against the bad bacteria against the invader. So are they doing more good or good? Doing more harm. And I don’t know either. These things have hardly been tested and the people who make them aren’t particularly interested in testing.
ZIMMER: So we should, we should just talk a little bit about. I mean, we’ve lot, I’ve been talking a lot about the gut, but the skin is covered in bacteria, right?
HANDELSMAN: And it’s a completely different flora than we have in our gut or our mouth or our ears. In fact, the two hands differ a left and right.
ZIMMER: So. And are they, are they, are they doing, are they doing good things for me right now?
HANDELSMAN: Yeah. They’re protecting your skin just like they protect any surface they’re on, they’re good guys. You have to get used to this respect for the microbes thing.
ZIMMER: Okay, okay, now I can handle this. And so, so if you use these sort of hand sanitizers with the antibacterials-
BLASER: There are times to use them in the hospital, it’s very important to use them because you have a lot of bad bacteria transmitting in hospitals. So washing the hands and a variety of different ways is important. And during flu season it’s very important because flu is transferred by people’s hands. But if you take all of that collectively, maybe that’s three percent of the time. The other 97 percent of the time, the benefit is just leaving our microbes alone.
HANDELSMAN: I think the biggest thing any of us can do is treat our flu symptoms very respectfully. Stay home, not, so you don’t transmit it, wash your hands with soap. Purell won’t help with flu, but uh, that much but certain, oh, well yeah, get get you saying get the shot. Get a vaccine. That’s right, and because I think more antibiotics are given for flu like symptoms that turn out to be viral, but we don’t have the test to prove that than probably any other disease, so I think if we kept the flu under control and that can be controlled just by behaviors and washing hands and breathing in people’s faces.
ZIMMER: When?
HANDELSMAN: Usually November or December till our early March events.
ZIMMER: Vince?
FISCHETTI: You have to realize that 90 percent of infections come in through the mucous membranes. They’re not coming in on your hands. They are coming in through mucus membranes. Your eyes, your your genital track. So when you touch something that’s contaminated, you’re not getting infected through your skin. It’s when you touch your nose, or you touch your mouth that the organism then gets it. That’s how it gets in.
AYRES: You have to have a wound. Your skin is a barrier.
FISCHETTI: The only other way is a wound. You’re bringing the organism from where the other, whatever you picked up and you touch your nose and how many times you touch your nose and your mouth.
HANDELSMAN: About 12 times an hour for the average person.
ZIMMER: Wow. In the back there.
AUDIENCE: I think multiple of you stadia, but you were basically because you were using bacteria. No, because you were developing and what do you got? Penicillin and all which came from soil bacteria and therefore the soil bacteria had natural built in resistance to the compound you were using. A question, is it possible to synthetically generate proteins or protein analogs which would bind to sites or would interfere in other ways with mechanisms for which things have not developed resistance to because they weren’t. They aren’t actually naturally occurring equivalent to penicillin.
ZIMMER: Yeah. That’s actually an interesting point is that I think they’ve done studies right where like they would look at old soil and actually actually find that there were some resistance, resistant microbes like before the invention of antibiotics.
HANDELSMAN: That’s right. They’re all over it. My, my group has studied a site in Alaska that’s essentially as pristine as you can find a site on earth and it has very little exposure to antibiotics and we find a large array of antibiotic resistance genes. We also have found that when, purely synthetic antibiotics had been introduced on the market, resistance has even faster in some cases than to the naturally occurring ones. Penicillin’s been on the market for what, 60 or more 70 years and it’s still useful. Some of the this synthetic antibiotics can’t even be used anymore because there’s so much resistance, so we’re dealing with evolution. I think that’s the answer to the question of why there’s no universal cure or prevention because we’re dealing with evolving organisms.
ZIMMER: So I guess the lesson is that bacteria are pretty awesome.
HANDELSMAN: They really are.
ZIMMER: All right. Well let’s give a hand for our panelists. Thank you for coming.