1,410,297 views | 01:25:32


![]()








What if your brain at 77 were as plastic as it was at 7? What if you could learn Mandarin with the ease of a toddler or play Rachmaninoff without breaking a sweat? A growing understanding of neuroplasticity suggests these fantasies could one day become reality. Neuroplasticity may also be the key to solving diseases like Alzheimer’s, depression, and autism. In this program, leading neuroscientists discuss their most recent findings and both the tantalizing possibilities and pitfalls for our future cognitive selves.
This program is part of the Big Ideas Series, made possible with support from the John Templeton Foundation.
NARRATOR: Our human newborn, Augie Nelson’s current abilities are somewhat limited. He can cry, sleep, eat and hiccup. The turtle, also newly hatched, can crawl, separate from her siblings and begin a vast trans-Atlantic migration, alone without parents or learning. Her brain has already formed every connection she’ll need for the great journey ahead. Seven months later, Augie is learning to sit up. In a year or so, he’ll be walking. Another decade, he’ll be walking to school by himself.
NARRATOR: By that time, the turtle will have completed a solo 9000 mile circumnavigation of the Sargasso Sea and returned to the shores where she was born to build her own nest. The turtle’s brain was designed to masterfully navigate the ocean, but Augie’s human brain was designed to adapt to any environment, play any instrument, calculate the existence of the space-time singularity, navigate the Atlantic by himself, if he wants. Everything he needs to learn these things is already there.
ALVARO PASCUAL-LEONE: We’re born with as many neurons and as many connections as you’re going to need. They can go from any spot of the brain to every spot with as many connections as possible.
NIM TOTTENHAM: That’s a brilliant design by mother nature because it gives us this incredible amount of possibilities for the future.
NARRATOR: But there’s a catch. That gift of possibility doesn’t last forever. Like childhood itself, it comes to an end. For each skill, we get a golden period when learning is easy.
TOTTENHAM: Periods in development when we have a heightened plasticity for shaping neural circuitry and we refer to those as critical periods.
PASCUAL-LEONE: Learning to play the guitar as a child is like opening a door and as a child, we have lots and lots of doors.
NARRATOR: During this time, our neural circuitry gets fine tuned.
TOTTENHAM: Our brain learns about which connections are going to be important through a use it or lose it principle.
PASCUAL-LEONE: Certain connections become reinforced and sustained and enhanced at the cost of others.
TOTTENHAM: Those connections that aren’t being activated because they’re learned not to be necessary, get pruned away.
NARRATOR: They actually die off, and the open doors begin to close.
PASCUAL-LEONE: As an adult, if you’ve never played, you’ve lost that door.
NARRATOR: So right now, Augie can learn to speak any human language perfectly without an accent, but when he’s an adult, he will have lost that ability. If he doesn’t begin learning the violin before he’s about seven years old, he’ll probably never play Carnegie Hall.
PASCUAL-LEONE: If you never had the connections to begin with, you can dry as hard as you can. You’re never going to get there.
NARRATOR: But what if we could change that? What if we could tweak our brains to learn as easily as a child? It’s called The Holy Grail of Neuroscience, and it is tantalizingly close.
PASCUAL-LEONE: We can, to some degree, do the impossible and reopen critical periods to say we allow changes to happen later on, in ways that we didn’t anticipate would be possible.
NARRATOR: Scientists are learning how we learn, and that may soon give us a chance to reopen those doors.
GUY MCKHANN: So what actually is neuroplasticity? Neuroplasticity is the ability of the brain to adapt to changing circumstances. To an environment changed, the ability of our brain to in a nutshell learn. But there’s another side of the coin. Just as we need to be able to learn to adapt, we also need stability. The opposite of plasticity, neuroplasticity, is brain stability. So in fact, that balance is what we’re going to focus on a lot tonight.
MCKHANN: Our first participant was the first woman to chair the Department of Neurobiology at Harvard Medical School. Today, she’s professor of Biology and Neurobiology at Stanford University. Please welcome one of the world’s foremost neurosciences, Carla Shatz.
Our next participant is Associate Professor of Psychology at Columbia University, director of the Developmental Affective Neuroscience Laboratory, Please welcome Nim Tottenham.
Our third participant this evening is Professor of Neurology at Harvard Medical School. An MD-PhD, he says his research falls in the area between the brain and the mind. Please welcome Alvaro Pascual-Leone.
MCKHANN: So welcome everybody. So Carla, let’s start with the brain itself. We’re going to be talking about learning plasticity, how the brain learns, how skills become habit. But what do these things actually look like in the brain structurally?
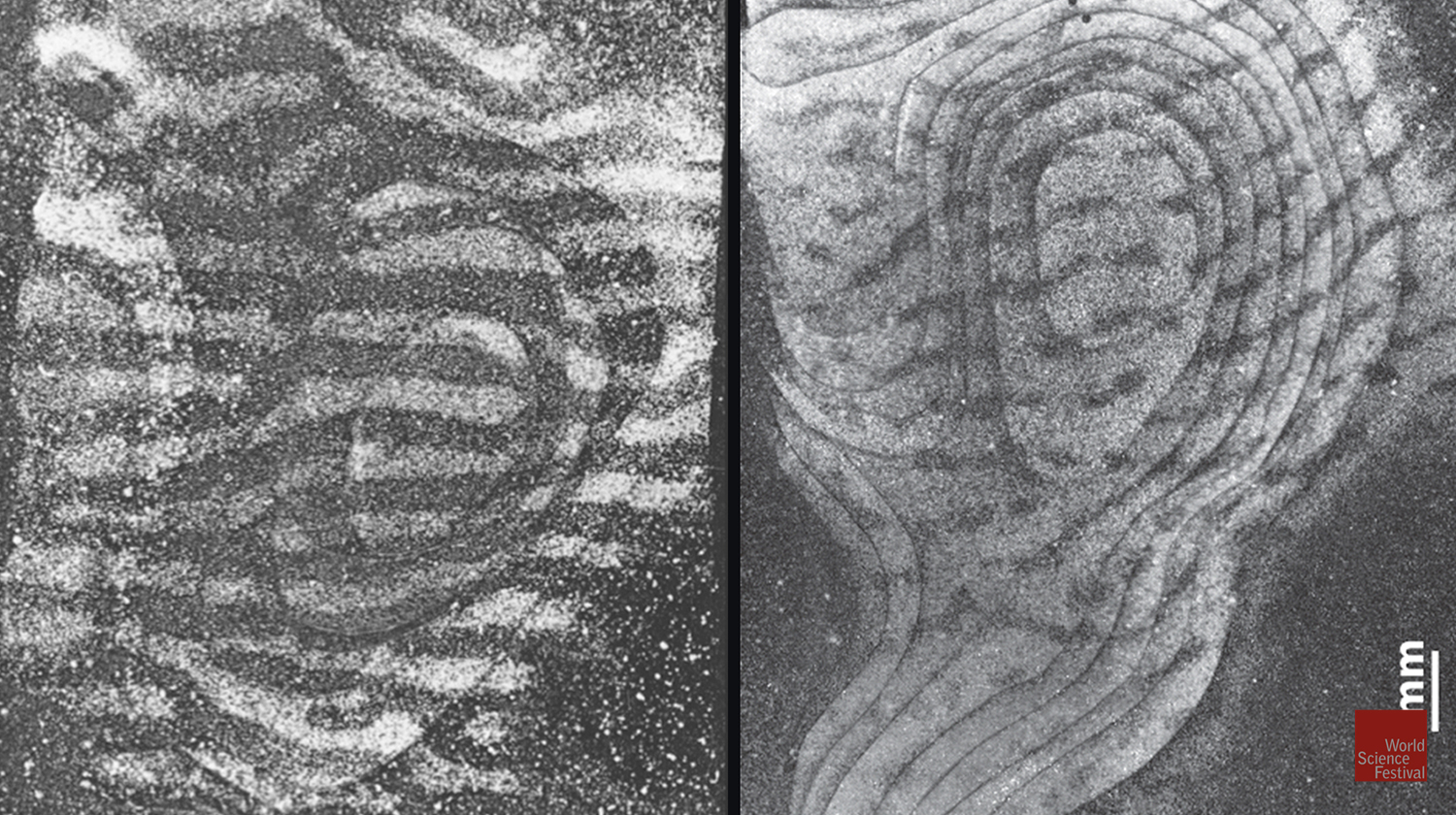
CARLA SHATZ: We saw already some nice photographs in the introduction, if you remember of these black things. Structurally, the brain is composed of neurons and support cells. The neurons communicate with each other through electrical signaling; chemical electrical signaling. The most important aspect of that is that these communications are transferred across structures known as synapses. That’s where learning happens. That’s where memories are stored, and as we were talking about in the video, that’s where the pruning, this pruning process goes on, this use it or lose it process goes on during development.
So, in fact, the structure of the brain is just the brain is packed with these neurons, packed with these synapses and also with very long connections. Some of those you can actually see in this beautiful graphic that’s being displayed now. So the brain connections link various parts of the structure to each other, ad those are the beautiful colors that look like Us and so on, these pathways. But those are made up of hundreds and thousands of connections from individual neurons. I used to joke there are more neurons in the brain than stars in the universe, but in fact, an astronomer corrected me and said that wasn’t true.
MCKHANN: So when you look at an amazing picture like that, we’re looking really at the axons, the wiring-
SHATZ: The wiring.
MCKHANN: Is the brain fundamentally un-wired at the start?
SHATZ: The brain is not fundamentally un-wired at the start. But it is amazing, if you just take the visual system, for example, the eye is not connected to the brain to start with. The nerve cells in the eye, have to grow their connections along pathways and select the right part of the brain, namely the visual part of the brain, not the auditory part of the brain or the motor part of the brain.
So the wiring from the very beginning is very highly organized and the formation of these long tracks or pathways is dictated by very strict cues like pathways or even like roads with street signs on them, so that these growing connections or the growing axons follow these pathways. But then the amazing thing is once the connections form between these long distant regions of the brain, then there’s this period of overproduction and pruning that we’re going to talk about. A period of extensive plasticity where the outcome is really predicted by the use of the circuit itself and the experience itself. So there’s both directed kind of hard wiring early, followed by this remodeling plasticity that happens later and really persists to some extent throughout life.
MCKHANN: So then building on that, if we think about it, if you’re building a house, you’re not going to lay copper wires all over the place and then pull out the ones that don’t seem like they’re working well. But that seems to be what we’re talking about. It seems pretty inefficient and the brain is 2% of the body weight, but yet gets 20% of the blood flow and 25% of the glucose. So why is the brain doing it that way?
NIM TOTTENHAM: Yeah, so on face value, there’s so much about brain development that seems inefficient, but actually it’s that seemingly inefficient path that actually gives rise to the incredible complexity of the brain, especially in the case of the human. So when we’re developing, what our brain does is first goes through this period of over producing our neurons and synapses and then through experience, through learning what’s important in the environment, what synapses are getting activated, those get to stay and everything else gets snipped away because it’s inefficient to keep all of those synapses.
So, why would we go through this entire process of over producing and then pulling back? That’s really at the core of what the function of childhood is in the human. So if you think about humans as a species, we’re amazing in many ways. We can live anywhere on the planet. We can speak any language, we can eat a number of foods and so on and live very well. Some of the reason why we can do that is because of this long period of brain development that we have. So the brain overproduces, it’s like throwing a big fishing net out into the ocean because you’re not sure which house you’re going to end up in. You’re not sure what language people are going to be speaking to you.
So you’re ready, you’ve got all your bases covered. Then depending on what signals are coming into the brain, the brain learns, “Okay, I’m going to keep the synapses, but I’m going to get rid of these. So if I’m growing up in a Japanese speaking household, I’m going to hang on to the synapses that help me understand Japanese, but get rid of the synapses that support other languages because that’s really efficient.” So it really is this developmental period, a really long one in humans, that gives rise to our incredible adaptation to our particular environments.
MCKHANN: So, Alvaro, is this a new concept? We all think everything’s been figured out in neuroscience in the last 20 years, but this need to balance stability and plasticity, tell us a little more about that, about the history of that conceptual.
ALVARO PASCUAL-LEONE: I think there’s lots of new developments, but many of the ideas are not fundamentally new, we have the tools to actually test the concepts. But the first person to speak about plasticity and stability as a term and apply to behavior; to human behavior, was Williams James; the psychologist Williams James in the 1890s. He wrote about plasticity as being the property for substance of an organ, presumably of the brain, that enabled us as humans to do certain behaviors and become really good at it. He was talking about behaviors, a habit, not about the brain structure. He said, the amazing thing, it has a property of giving in to influence but not giving in all at once. You want to have some plasticity but not too much plasticity. You want the right kind of plasticity, the right amount of plasticity.
Presumably, it was Ramonica Haldane, not much longer, who started to look into where does that actually happen in the brain and describe the synopsis and the changes in the connectivity and the change of how efficacious those connections were in making new ones as the substrate for that plasticity that Williams James was talking about. So the ideas are 100 years old, and yet when I was studying medicine, I was told, “Things don’t change in the brain and when you get old, well tough.” I thought, God, I hope we can do something about it because I hope to get there one day.” I think we start and all know, we’ve always known, as an old dog, you can still learn new tricks. It was against the experience of everybody that it is possible to learn new stuff. So how does that gel together?
MCKHANN: Great. So now let’s go back to this. We were talking about this concept of a critical period. We all know the old adage that children learn language a lot more easily than adults. But what are some of the other examples of critical periods that you see in your work with children?
TOTTENHAM: So for a while, people were thinking that there is a critical period of human brain development that was the language that people used and then it became clear that critical periods are really a property of a developing neural circuit. So if that’s true, then maybe it’s appropriate to think of each neural circuit that we have as undergoing its own critical period. That moment, the metaphor that people often use for a critical period is that it’s a window of opportunity opening up when the environment can really have its biggest impact on the nature of future functioning for that system.
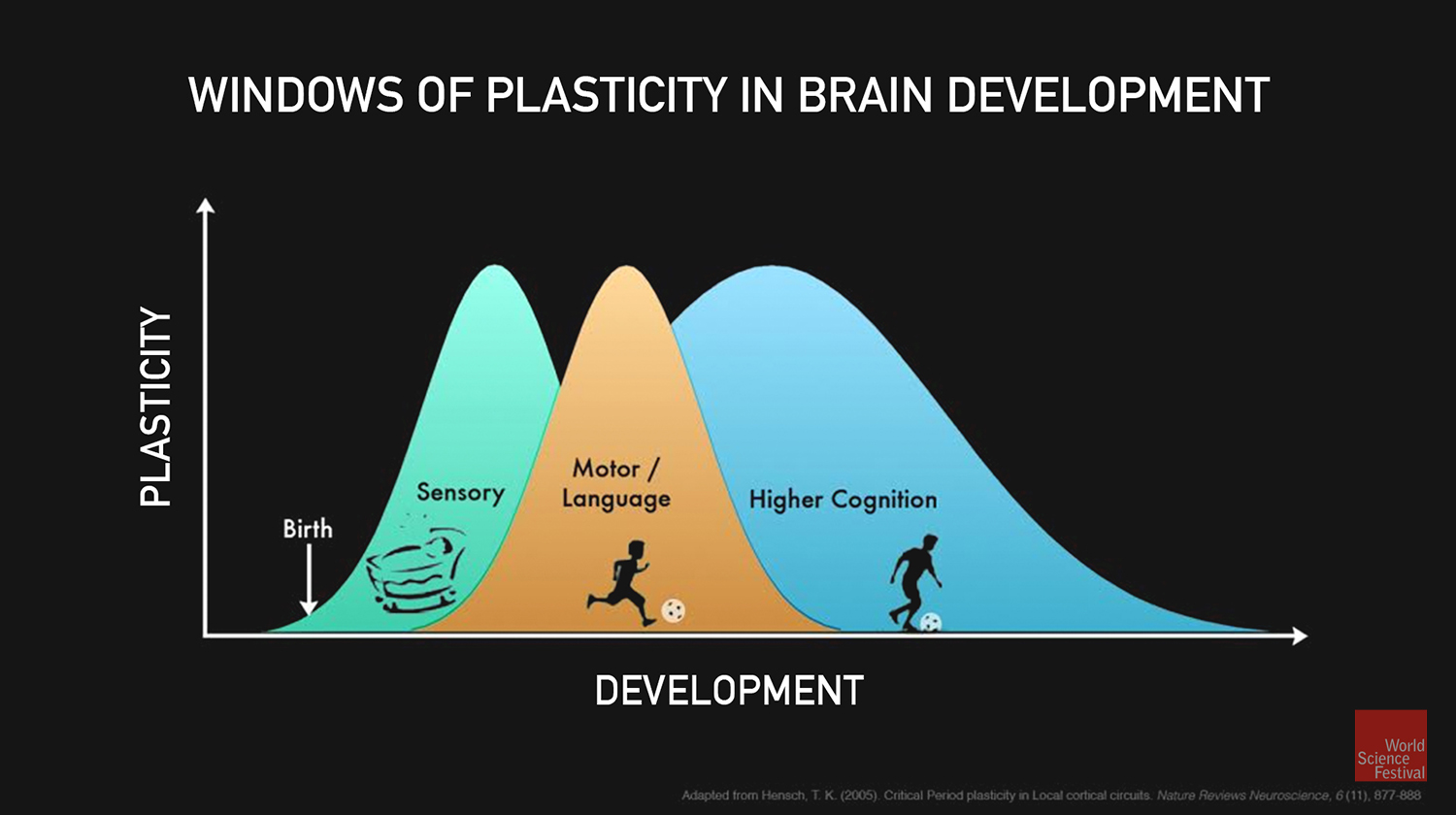
If it’s true that every neural circuit has its own critical period, then maybe we can sort of map out the timing across the brain. So in general, what people find is that the brain develops in this backwards C-shaped nature where regions of the brain that are low and back tend to develop earlier, then the development curls around in waves.So what you often see, sensory systems develop earlier, experience their critical periods, followed by motor systems and language systems, and finally more of these higher cognitive functions that particularly in the human, we spend so much time thinking about. So, things like our emotion processing or our cognition, academic performance and so on. So, that hierarchical structure really makes sense when you think about what the needs of the developing infant child or adolescent are going to be.
MCKHANN: So the video, we saw a baby turtle that really doesn’t have a childhood. It jumps in the ocean and takes off whereas humans, we have this extended childhood period where all of this has to happen. You could argue that because we have the most to go through experientially, that we have the longest childhood.
TOTTENHAM: I think it’s another good example of what seems like an inefficient design, right? So if we’re going to stay and mature for that long, then we need somebody around us who’s willing to put in the investment to stick around with us that long. So if you look at this immature period in the human, it’s really a long time, right? In most species, this period of immaturity is on the order of weeks, maybe months. In humans, it’s years.
So that’s a curious design from mother nature to come up with because it’s a huge energy suck for a parent, right? To raise another human being. I don’t remember, I don’t know what the numbers are, but someone computed how many calories it would take to raise another human being and it’s enormous. So there’s gotta be a really big payoff. One of the arguments is that the payoff is that this affords us as a species, this incredibly long period of plasticity so that we can do all the learning that’s necessary to become a very complex adult.
PASCUAL-LEONE: So at the same time, I think what we’re learning is that there’s this notion of development and then you get to some level of maturity, which I’m still hoping for, and then you have a plateau and at some point things go wrong and if you are unlucky, you start losing it. This way of thinking about it is probably the wrong way to think about it. That, instead, we should think of us developing our entire lifespan until we sort of die and that therefore plasticity, even though it may be through different mechanisms and different efficacies and working on different substrates, but it’s still there.
It’s still there throughout the lifespan. So it’s not a critical period in the sense that plasticity is done and now you can reactivate plasticity. You can open opportunities, but the capacity of change, balancing the stability is there for the entire lifespan, which is from a neurologist’s point of view or neurosurgical perspective, a huge opportunity and reason for hope and of interventions.
SHATZ: This balance between stability and plasticity is really interesting. If you just think about some of the systems that have to form, then you don’t want necessarily plasticity throughout life in a system, let’s say, like our visual system where we need to have a stable representation of the world inside our brain. Then we can draw upon that to make computations to put together and to have perceptions and so on.So it’s really quite interesting. So some systems really need to go through this learning period, but then to become more stable than other systems.
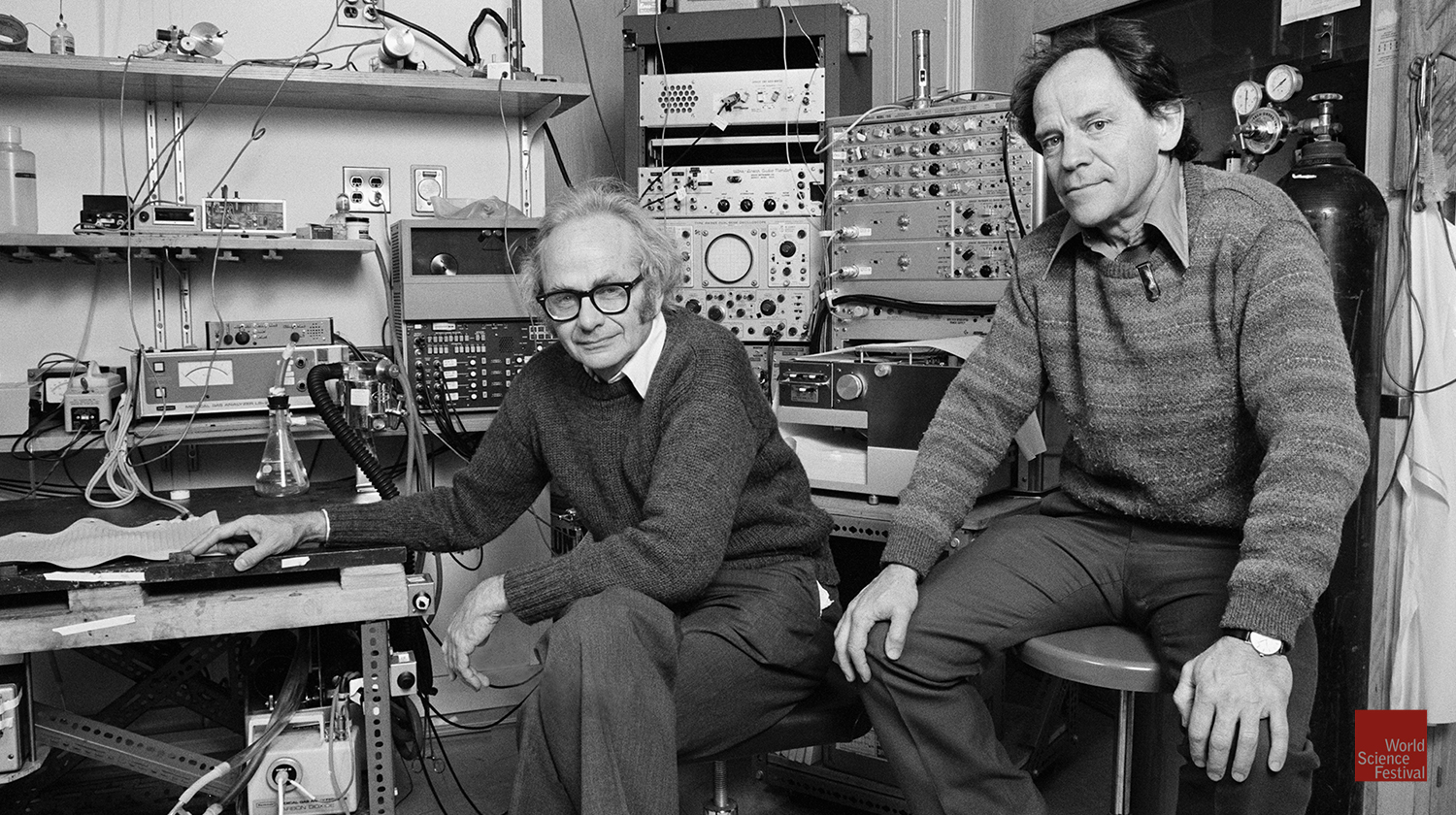
MCKHANN: So let’s let build on that a little Carla, because the visual system, your mentors at Harvard, Hubel and Wiesel won the Nobel prize in 1981 for their fundamental work on really the first insights into all this concept and the visual system. So help us understand that a little more.
SHATZ: Oh, sure. So, this is David Hubel and Torsten Wiesel. My mother … I used to call them Hubel and Wiesel and my mother thought it was a person, one person Hubel and Wiesel, till she met them. But yeah, so these two wonderful scientists explored the visual system and began to try to understand how it is, well, here’s the question. How come we see with one view of the world, even though we have two eyes?
So both eyes have complete circuit. It’s like you have two cameras. I mean, both eyes bring complete images of the world to the brain, yet unless there’s pathology, we only see one view of the world. The answer to this as both in the wiring of the connections and also the fact that the brain has to learn how to use both eyes together. It does that during a developmental critical period. So the connections from the two eyes begin to be mixed together as the connections move from the periphery, from the retina itself into the central nervous system. The first binocular cells are actually built in at the back of your brain in your occipital cortex. That’s your primary visual cortex.
But even though the connections know to grow to the visual part of the brain, they actually don’t know how to tune up to make binocular neurons. One way they do that is to interdigitate the connections between the right eye and the left eye into a series of beautiful right eye, left eye, right eye, left eye stripes. You’ll see two images here actually. So there’s an image where there are white and black stripes and those stripes are equal in size-
MCKHANN: On the left.
SHATZ: On the left. Then there’s another image on the right where there are little teeny black holes in the middle of a sea of white. Now what you’re looking at, let’s just say on the left, every little white dot is the size of about a synapse. So one of these connections and you’re looking then at literally millions of these connections. What you notice is that they’re beautifully organized in the stripes. When Hubel and Wiesel first discovered this intermixing of the two inputs, which are essential for making the binocular neurons, everybody thought they were hardwired.
But they did a very important experiment. The experimental result is on the right. Let me tell you about it in just one other context, which is really to talk about the mystery of the cataract. So you know perfectly well if as an adult you have normal vision your whole life and you get a cataract as an adult, you lose the vision in your eye because there’s a clouding of the lens. Then a miracle can happen. That you go to the surgeon and he replaces the lens with a clear lens and you see beautifully again, immediately. This replacement could happen after maybe 10 years of not being able to see well through your eye.
Now, in contrast, a little child who might be born with a congenital cataract or have some other problem with vision in one eye, if that cataract is not a corrected immediately, then that child will be permanently blind or have severe vision loss in that eye. So what’s the difference? My grandma had a cataract, 10 years worth, corrected, good vision, and then the child maybe has a cataract just for a year, maybe even half a year, and it’s corrected, the optics of the eye are corrected, the camera works, but the brain can’t see. So what’s the difference? Hubel and Wiesel did an experiment where they actually checked the connections between the eye and the brain that was shown in the right hand side.
The open eye, the white eyes connections take over way more than their fair share of cortical circuitry for vision. The closed eye has those little piddly black holes. This was an amazing demonstration, a very important demonstration, in fact, the first of the use it or lose it concept in the brain. That the brain connections require use in order to be maintained and in fact even require use in order to be formed.
MCKHANN: So can you go into a little bit how you’ve been building on that work? I think you’ve got a video for us of how the brain does this in real time?
SHATZ: This really illustrates a developmental critical period that happens after birth. But actually, we were quite interested in knowing whether there are earlier developmental critical periods in the visual system. What we discovered is that even before babies are born, the eye is sending signals to the brain to start to really shape up these beautiful stripes and these connections in the central pathways. The signals are the electrical signals that are being sent from the neurons in the retina into the central part of the brain. They’re actually like test patterns, they’re at testing the connections, and the ones that are appropriate are being maintained and the other ones are being pruned away. So this is the same theme.
The video that you see now is a picture of that signaling process in the eye. So you can just imagine it’s like phone calls being placed to the brain really early in development and every little black dot here in this video is again about the size now of a nerve cell, not a synapse. So it’s a bigger scale, but you can see that whenever … when the cells become black, it means they’re placing the phone calls and they’re sending their signals to the brain. So, what you’re seeing here is neighborhoods of nerve cells, all placing phone calls together.
This is actually part of another principle of development, cells that fire together wire together. So this is a way that the eye can test to make sure the connections are orderly in the target structure. This is happening. So the brain is really jump starting vision even before vision is possible because it’s in utero, and it’s before the rods and the cones have appeared. Now that we know that this happens in the visual system, it’s been found that this kind of jump starting and testing is happening all over the brain during development, very early development.
MCKHANN: You’ve been studying ways to potentially reopen the visual system. So tell us about that a little bit.
SHATZ: Yeah. Well, the question is really if these windows close, can you open them up at any time? And really to try to understand how to do that, it’s important to know something about the molecular mechanism. So what are the molecules that are opening and closing these developmental critical periods? And really in particular, what are the molecular mechanisms that control the pruning process itself, this selection process, which synapsis should we keep? How does the brain know that certain synapses have been used and they should be strengthened and other synapses have not been used so much, so we don’t need them, so we can actually prune them away?
So we can use animal models to begin to discover those molecules for pruning. In doing that, in fact, we found a number of candidate molecules that we wanted to test to see if they were important for this pruning process. We engineered genetically mice that lack these molecules to see what would happen to their critical periods and to pruning. To our great surprise and delight, what we discovered is that if certain of these molecules, when they’re not there, permit the persistence of the developmental critical period in the visual system and in fact pruning fails to happen. So this is illustrating two points. One is that it is possible to continue to extend a critical period for a longer period of time. It also indicates the idea that brain plasticity itself can be regulated in a very deliberate way, and if we only knew the whole story about the molecular mechanisms, we really could make pills and I could take a pill as an adult and learn French without an accent.
MCKHANN: So that brings up an interesting point because Alvaro is over there smiling and shaking his head. So as a clinical neurologist-
PASCUAL-LEONE: I’ve taken the pill, exactly.
SHATZ: No, but would you want to take it right away?
MCKHANN: As a clinical neurologist and you think about that and we talk about the balance between stability and plasticity and as you’re taking care of patients with strokes and things like that, what do you think about in kids as … Well, ’cause everybody’s obviously going to, “Well, we got to get these into humans. We’ve got to figure out ways to extend these windows for kids and for disease to adults.” So let’s talk a little bit about the pros and cons of that.
PASCUAL-LEONE: Yes, I think it’s a really important topic and it is a double edged sword. So to have a great efficient plastic brain that is able to get us to learn French or English without an accent, it may be very appealing. But at the same time to have too much plasticity can come with a cost. If you have, not in a genetically engineered mouse, but a disease where by design, because of their pathology, the brain is too plastic, is learning too fast, and that seems at face value a great thing. You’re able to acquire skills that go above the average one of us.
You can open up a box of matches, have them fall on the ground and say 27 and be right or 225. You can learn a whole book of names and phone numbers and we call those savant abilities. It’s sort of cool and it’s certainly partly a joke. But it comes to the course because what happens to the brain is that normally it yields to influence to the environmental change. Then we stop and then we experience a new thing and that new thing falls on to fertile grounds, ready to learn the new thing. But it doesn’t get colored, but what we just learned.
The risk of having too much plasticity is that the brain is change and then the change falls on to the change and the change into the change and the change … it is often a messy, noisy system. We think that for example, diseases like autism are characterized by excessive, too good at plasticity, that leads to a failure of pruning and to a developmental disorder because of the number of [inaudible 00: 35: 24] plasticity. So to have too much may be a bad thing.
MCKHANN: So you’ve been studying that in autism specifically to try to look at plasticity in the autistic brain versus in the neurotypical non autistic brain. So what do you find, how do you go about teasing that apart and what do you find?
PASCUAL-LEONE: You have to come up with experiments is it worthy to show that people with autism can be better at learning for example than the individuals that are not autistic? And things like learning a sequence of finger movements that repeat themselves by doing it to figure out the pattern underneath the finger movements. Individuals with autism learn to do that faster than those without autism. But if you have one pattern followed by another, then they break down because they run into interactions between the two things that they are learning.
At the same time, we want to look in the brain and see what is changing in the brain to allow them to learn these skills faster. We do that in a similar way, that we’ve learned to do it in animal models or in slices of the brain using electric stimuli to evoke a response and then using trains of little stimuli to modify those connections and see for how long they remained modified. We use that using a technique called transcranial magnetic stimulation.
MCKHANN: So tell us a little more about that technique and how you’re able to use it noninvasively to test something like this. To perturb the brain transiently.
PASCUAL-LEONE: It’s a bit like science fiction. It’s still to me. You basically put a coil of copper wire over the subjects head then as the current passes through the copper wire coil, it induces a current that goes through the skin and the skull and induces a current in the brain. Maybe we can show it and it has a little explanation that goes with it.
NARRATOR: TMS stands for transcranial magnetic stimulation. It is a way of inducing current in the brain. You need specific controlled part of the brain without having to open up the skin and the skull. It turns out that when you apply repetitive stimuli, then you’re activating a zero grid over and over in your control pattern, and that changes that [inaudible 00: 38: 07] zero grid. So that allows us to activate, probe, disrupt or suppress activity in different parts of the brain depending on where we target and what parameters of stimulation we applied.
PASCUAL-LEONE: So you can probe the brain with this technique, see the response, apply a little train to modify it. Then what you find in people with autism is that the effect of that modification lasts literally longer than it does in neuro-typical subjects in those without autism.
MCKHANN: So Nim, we’ve talked mostly and now we’ve talked about vision and we’ve talked about motor system. You study a lot more aspects of emotional phases of development. So let’s talk about how you’ve been studying that in these exact same context of plasticity and stability.
TOTTENHAM: A lot of our questions are related to the point I made earlier that we have this design of spending a lot of time with our parents while we’re growing up. So we have been very interested in the role of the parents during this putative sensitive period for emotional behaviors. So, we know since the time of Freud, that there is this very strong association between early caregiving experiences and emotional behavior later on in adulthood. But we don’t really know at the level of human brain development why that enduring link exists. Part of the answer may have to do with some of these critical period timing and the influence of the parents. So we’ve been asking questions about, actually, what good is a parent? We know that parents are important, but what are they actually doing on a moment to moment basis? As I’m rushing my kids out the door to school, shoving breakfast into their mouths to get them out the door, what are those momentary episodes important for?
But we also have the opportunity to ask questions about children who experience more forms of adversity early in life. The reason that we’ve been very interested in this group of children is because this early adversity exposure is one of the number one preventable risk factors for emotional difficulties later on in life. We’re just at the beginning stages of understanding why early adversity in particular is so important, maybe more important than later adversity. Part of the answer is related to the concept of critical periods that we’re talking about.
So you brought up the idea of a double edge sword before. I think that there are many double-edged swords when it comes to brain plasticity. Another one of those is that brain plasticity is not really good or bad. It just is. It just opens you up to the environment. So when considering or evaluating brain plasticity, it’s also important to look at what’s the nature of the environment that the individual is experiencing when the brain … when that window of opportunity is really open.
So for children that have experienced significant adversity, like caregiving adversity or what we often call psychosocial trauma, what we have seen, well, two main things. One is that there’s incredible individual differences in outcomes. So some children show some really significant challenges and others are thriving. So this is an individual differences story that we really aren’t very good at explaining right now.
But the other piece that we’ve been seeing, and this is true not only in humans but across a number of species, is that early adversity may actually be affecting brain development on average by affecting the timing of these critical periods. So there may actually be an acceleration of the timing or the opening of these critical periods. So if we know that, that’s really important to know in terms of intervention and prevention, because if the timing of these critical periods are shifting as a function of early experience, then that informs how we want to treat individuals and what new experiences we want to give to individuals as a function of these early experiences.
MCKHANN: And that’s why you like to refer to these, as you said before, as sensitive periods, more than critical periods.
TOTTENHAM: For the processes that we’re interested in, these emotional behaviors and cognitive behaviors, that seems to make more sense to me because they do seem to be more malleable. In fact, that’s why talk therapy is supposed to work. Is that talk therapy is about teaching the brain something new about interpersonal relationships. The reason, the only way that talk therapy can work is if there’s continued plasticity in some of these systems.
MCKHANN: So we talked a little bit about autism. Let’s talk a little bit about schizophrenia because they’re another very complex condition and there are questions about whether or not schizophrenia may have aspects of a disorder of stability and plasticity. So, Carla, maybe you could enlighten us on that a little.
SHATZ: Well, I mean, one main point to make about schizophrenia is that it’s not really commonly considered to be a developmental disorder. Even though often symptoms appear late in late adolescence or even beyond, the current idea is that there’s this extended developmental critical period and this period exists beyond the visual system as Nim has mentioned.Therefore, these systems that are maturing much later, including those that have to do with interactions and with cognition and frontal lobe behavior, all mature later. So then the question is what are the changes that have happened in the brain?
Again, it’s commonly now thought that this relationship really between plasticity and stability must be perturbed in some way. When people look into the brain of a … not a huge amount has been done, but there is consensus that there are changes in pruning in the brains of schizophrenic patients who have donated their brains for studies so that we can actually look at those brains. In human genetic studies we’re looking for susceptibility genes that might produce schizophrenia in children, some of the new gene candidates that have been identified are known in animal models where we study how those genes actually work, are known to regulate pruning in the animal, like the mouse developmental critical periods.
So, now you’re beginning to hear a kind of common theme that’s emerging as we talk, that there are these critical periods that involve a beautiful balance between plasticity and stability, involve pruning and may have different outcomes, not only through our own experiences, but also when the balance somehow is disrupted by some kind of pathological condition.
GUY MCKHANN let’s talk a little bit about how do we harness recovery of damage after injury. You talked a little bit, Nim, about a traumatic situation, but what about critical periods in childhood, when we get to adulthood, how do we attack that problem?
PASCUAL-LEONE: Well, I think the way we’re talking about plasticity really say it’s a huge reason for hope, right? It suggests the fact that our brain can be guided and the challenge is to learn exactly how to guide it. What do we need to do to suppress changes that are these double edge sword that good cause problems and to enhance others that can benefit the subject? We have lots of interesting indications that that is possible to do. Ultimately, that’s what physical therapy, what occupational therapy, what speech therapy promotes. Is the talk therapies guide the changes for the benefit of the subject.
But I think we have now as we understand more of the molecular basis and the physiologic basis of these mechanisms, we have ways to target these mechanisms with medications or with devices, with brain simulation that more directly to the brain promote the changes. That’s happening and it’s happening guided by basic research and translating that basic research to humans. So … sorry.
TOTTENHAM: One of the things that I’m really excited about in terms of intervention is thinking about how can we boost the power of current interventions by knowledge about critical periods in plasticity? So if we can increase plasticity prior to some known effective intervention, that’s really powerful. So, as you mentioned, there are many examples in basic neuroscience where pharmacologic or genetic administration or modification can actually increase plasticity, and in many ways, bring the brain back to that childlike state to allow for some environments to have a really big effect on the brain.
That’s really powerful and there’s a demonstration in humans too that has actually used one of these pharmacological manipulations with people who don’t have perfect pitch and perfect pitch depends on critical period learning early in development. So perfect pitch was able to be developed in adults who had taken this pharmacologic drug. So then the question is, well, why don’t we all do that? Right? The authors of the study make a really … they’re very careful to say that, “Hey, remember the brain actually spends a lot of energy to prevent these critical periods from opening up again.”
The brain wants efficiency, the brain wants reliability. Do we want to remove all of the lessons that we’ve learned throughout our entire developmental history? Do we want to remove aspects of our personality and so on? So it becomes a very tricky question even though there’s a lot of promise for recovery following any type of trauma.
SHATZ: But in that perfect pitch study, they didn’t … the people didn’t lose … I mean, they learned something new. So there’s hope really. There’s hope for having a selective intervention. I think that’s exciting. I mean, from the animal studies. So, from looking again at the mice … and actually one of the authors of that study also has done work looking at the mouse critical periods for vision as has my own lab.
What we find is that you can actually go into the adult mouse brain and really restore juvenile plasticity in the adult brain. The mechanism of doing that seems to be, again, to allow for new synaptic connections to form. If we study the story of the childhood cataract, but now in the mouse, then remember I told you that if children have a cataract and it’s not immediately operated and, and clear optics restored, then they become either permanently blind or that vision is seriously diminished in that eye.
And really there isn’t a good way of treating that blindness, is called Amblyopia, in adulthood. But in these mice, one can actually make the cataract model and then go in the adult mouse, and engaging these childhood mechanisms of plasticity a effect recovery of vision in the eye that was blind, which is amazing. It’s really … demonstrates, I think, that by understanding the underlying mechanisms that regulate these developmental critical periods, it’s possible to go in and then to manipulate them again. To me, it demonstrates another thing, which is that there must be in the adult brain and presumably in our brains too, ’cause we have the many of the same molecules that are being studied in the animal models, there must be brakes on plasticity because these manipulations essentially take the brakes off and then of course you can worry about stability.
So then we come back to that, this whole theme. Again, but the idea that there’s actually more plasticity in our adult brain that we can tap into, to me is really exciting because you could say that even if there are some downsides, that after a stroke or damage to the brain, wouldn’t it be wonderful if it were possible then to tap into that latent extra plasticity even briefly and combine it with training and physical therapy. So somehow a pill that would let me speak French without an accent could actually have a really important therapeutic value, which would be to really help people recovery from brain damage.
MCKHANN: Well, what we have here is a video of a modern rehabilitation technique with a split treadmill. Maybe, Alvaro, you can tell us about the concept behind this.
PASCUAL-LEONE: Yes. So part of what physical therapy interventions like this or like something called constraint therapy that some of you may have heard about it in individuals that have stroke, that cannot use both legs in walking correctly or cannot use one hand correctly, we’ve come to learn that if you force the use of the other hand, of the impaired hand by limiting the default of just using the unimpaired hand or by in this case of the video, if you force the walking correctly by aligning the paretic leg because it cannot cross over, so, therefore limit the pattern of abnormality that normally would happen, that because of this repeated training doing the right thing, that promotes the rewiring that promotes the plastic change and speeds up the recovery.
So you can, by guiding, by constraining the behavior, use that as a way to improve the recovery process. So the opportunity of opening up the mechanisms of plasticity in such a way that they become more active and therefore benefit from the intervention more, becomes really appealing. Examples of that do exist even in humans, not only with medications. One of the things that we know about Alzheimer’s dementia, Alzheimer’s disease is that before the clumps of this abnormal protein come together and deposit the plaques in the brain, they are floating around. In that stage already they alter and damage synapses. So they become damaging substances for the mechanisms of plasticity as it were. If you take patients with Alzheimer’s disease and you try to get them to learn from video games or computer games and get better at cognitive tasks, they derive very little benefit. It would take too long to get a benefit that is sort of meaningful.
But if you activate that zero grid with brain simulation, for example, just before they actually engage in the cognitive training, now you get more benefit from the cognitive training. So combining interventions, device base pharmacologic interventions with behavioral interventions, I think is really a way to leverage what we know about the mechanisms of plasticity in a way that translates into benefit for patients.
MCKHANN: So we’ve talked a lot about aspects of disease and repair. What about this Holy Grail idea? What about the idea of actually enhancing the brain? Whether one day I was thinking, “Today, I had a long day,” and I was thinking, “Oh my gosh, I got to focus on what we’re doing tonight,” and I jumped in a car and when is the helmet going to come out through the ceiling or already being built into the roof where I can say, “If I can just get my temporal lobes going and my memory working a little better, how great that would be.” How far off are we? How far off are we from everyday enhancement of function?
PASCUAL-LEONE: It didn’t work this morning exactly.
MCKHANN: You were in the wrong car.
PASCUAL-LEONE: I was in the wrong car. I mean, what gave me pulse is that of course there is a lot of industry investment and really direct to consumer devices already claiming that that’s possible, that we don’t need to wait at all. That you can just do it today and you can build your own brain stimulator devices and then build it into your car if you want to. People will claim and try to convince us that it is possible to enhance capacities. The problem with a lot of those data is that what they show is that it’s possible to get better at performing a given task, not to actually get better at the fundamental skill that underlies the task.
So, I think that the attempt to get us there is already here, but we need greater understanding including greater understanding of that double edge aspect that Nim was mentioning.If we get better at one thing, will it be without a cost? Will the brain allow you to improve something at the cost of something else. So, for example, you can ask a question and say, “What if we were able to get better at paying attention to this part of the world? We know a lot of what the circuitry is, that allows us to pay attention to this particular spot.”
So you can actually identify those brain areas in humans, apply simulation that increases activity in those brain areas, and you can make people get better attending to this part of the world. But when you do that, it comes at the cost of attending to this part of the world. In fact, it does so because these two areas sort of … I almost say it is a yin yang kind of a relationship.So there are interactions between the two hemispheres. So if you improve one, you worsen the other. That’s easy to test in something as concrete as spatial attention for a visual task and something that’s complex as overall behavior or more higher order cognitive functions. What exactly the cost might be, is much, much harder to test. I think it raises not just methodological and biological questions, but real ethical questions. If you want to improve certain skills, what would potentially be the downside of it?
MCKHANN: What about memory? I mean, memory is something … to varying degrees, we’re all here, slowly moving along chronologically and everybody worries about what’s going to happen to your memory. In my world, people have the ability to sometimes put electrodes into the brain. That allows us to stimulate the brain and there’s a number of reports of different parts of the brain, if you stimulate at just the right way, you can make somebody’s memory performance better.
How do you think of that, as not a way to combat aging per se, but to help people adjust as they get older and keeping memory intact? Forget about super memory, even just trying to keep memory intact as we go along. How do you guys see us approaching that?
TOTTENHAM: I mean, correct me if I’m wrong, but aren’t there less sexy, innovative ways that people think about or have studied to enhance some of these processes? So, for example, the things that we know we should do, like getting good sleep, exercising. Engaging in cognitive stimulation throughout a lifetime have been associated with better cognitive aging in the long run. So those are hard things that we all know we should do, but routine things that we should be doing that may actually be improving some of this retention over the long term.
PASCUAL-LEONE: So lifestyle modifications do work and do work through plasticity. So physical exercise promotes cognitive function. In fact, if you do an analysis of all the studies that have been done in the literature which we just did, just published in … there is a … I don’t know why this is the number, but there is about 52 hours a day, 52 hours …
MCKHANN: Talking about enhancing…
TOTTENHAM: It’s really hard work.
PASCUAL-LEONE: It’s really hard work. 52 hours in six months actually. So it’s not a lot and it doesn’t matter how many hours per day you do it, it’s sort of a total amount of dose almost. But you need to put in some hours but it’s not a ton of hours-
TOTTENHAM: Of exercise?
PASCUAL-LEONE: Of physical exercise that improves cognitive function in the elderly. So I think that there is an effect of physical exercise onto the brain and it appears to be linked to mechanisms of plasticity, at least as one can probe them in humans with brain imaging and brain stimulation techniques. But I think rather than getting at the level of suggestions, you should sleep better, avoid medications that are bad for you, eat the right thing and the right amount and exercise and challenge your brain with new things and have social relationships.
All those things are true, but we should be able to get to enough understanding that we can prescribe it, that we can tell men, “This is the number of hours of this exercise that you need to do and here’s how we’re going to help you actually convert this hopes into realities.” Because it’s hard to stick with a program like that. So I think that’s the step that we still don’t have, is the understanding of how to actually make this a prescribable intervention, like we do with medications. We don’t tell patients, “Take something for that.” We tell them what to take and how much and so forth. So I think we need that level of understanding.
MCKHANN: But what about, Nim, happiness set points? Everybody wants wellness. Is it possible that we’re going to someday understand the brain well enough to say, “Okay, you’ve been through a really terrible life trauma, but we can actually help your set point.”
TOTTENHAM: Well, I would think about sort of maybe not happiness, but that feeling of being able to regulate your emotions, to be able to feel less sad when you want, to be able to feel more sad when you want. To have that emotion regulation ability. So there are studies, for example, with people who meditate, which we generally think of as a healthy lifestyle practice. But there are different levels of expertise in meditation. So there are Buddhist monks who do this for, say 40,000 hours in total versus really, really dedicated meditators who might’ve done this for 20,000 hours, and then novices. This research has shown that the amount of meditation practice, practice being the keyword, that the behavior has to be routinely engaged with, is associated with brain changes in the regions of the brain, like the prefrontal cortex that we know are associated with emotion regulation.
What’s interesting in that finding, and it relates back to the original walking example and the quote about habit, is that there was this inverted U-shaped dose response function such that the individuals who were meditating a lot but not to the degree of the Buddhist monks actually had the most different prefrontal cortex activity and then it came back down again for the Buddhist monks, suggesting that there is this element of plasticity in the brain regions that we know are associated with emotion regulation, but an element of habit can come into play as well, so that it starts to become more of a naturally occurring state of the brain that can be, as you were referring to before, the core process that’s being affected rather than the more superficial.
MCKHANN: So I would have to say in summary, that obviously we have a really, really tight balance between plasticity stability. But as we’ve all learned, they’re incredibly exciting things, not just normal behavior, attacking diseases going down the road.
But in the meantime, eat well, sleep well, meditate once in a while, exercise a whole lot, and surround yourself with really smart people who make you happy. For that, I thank all of you.
What if your brain at 77 were as plastic as it was at 7? What if you could learn Mandarin with the ease of a toddler or play Rachmaninoff without breaking a sweat? A growing understanding of neuroplasticity suggests these fantasies could one day become reality. Neuroplasticity may also be the key to solving diseases like Alzheimer’s, depression, and autism. In this program, leading neuroscientists discuss their most recent findings and both the tantalizing possibilities and pitfalls for our future cognitive selves.
This program is part of the Big Ideas Series, made possible with support from the John Templeton Foundation.

Guy McKhann has over 20 years of experience as a neurosurgeon/neuroscientist at Columbia University/New York Presbyterian Hospital, combining clinical skill and compassionate care to maximize patient outcomes.
Read More
Carla Shatz has broken new ground for women in neuroscience. At Harvard Medical School, she was the first woman to receive a PhD in Neurobiology and the first woman to chair the department. Her research aims to understand how early developing brain circuits are transformed into adult connections during developmental critical periods.
Read More
Nim Tottenham, PhD is an associate professor of Psychology at Columbia University and director of the Developmental Affective Neuroscience Laboratory. Her research examines brain development underlying emotional behavior in humans.
Read More
Alvaro Pascual-Leone is Director of the Berenson-Allen Center for Noninvasive Brain Stimulation and chief of the Division of Cognitive Neurology at Beth Israel Deaconess Medical Center. He is an associate dean for clinical and translational research and a professor of neurology at Harvard Medical School.
Read MoreNARRATOR: Our human newborn, Augie Nelson’s current abilities are somewhat limited. He can cry, sleep, eat and hiccup. The turtle, also newly hatched, can crawl, separate from her siblings and begin a vast trans-Atlantic migration, alone without parents or learning. Her brain has already formed every connection she’ll need for the great journey ahead. Seven months later, Augie is learning to sit up. In a year or so, he’ll be walking. Another decade, he’ll be walking to school by himself.
NARRATOR: By that time, the turtle will have completed a solo 9000 mile circumnavigation of the Sargasso Sea and returned to the shores where she was born to build her own nest. The turtle’s brain was designed to masterfully navigate the ocean, but Augie’s human brain was designed to adapt to any environment, play any instrument, calculate the existence of the space-time singularity, navigate the Atlantic by himself, if he wants. Everything he needs to learn these things is already there.
ALVARO PASCUAL-LEONE: We’re born with as many neurons and as many connections as you’re going to need. They can go from any spot of the brain to every spot with as many connections as possible.
NIM TOTTENHAM: That’s a brilliant design by mother nature because it gives us this incredible amount of possibilities for the future.
NARRATOR: But there’s a catch. That gift of possibility doesn’t last forever. Like childhood itself, it comes to an end. For each skill, we get a golden period when learning is easy.
TOTTENHAM: Periods in development when we have a heightened plasticity for shaping neural circuitry and we refer to those as critical periods.
PASCUAL-LEONE: Learning to play the guitar as a child is like opening a door and as a child, we have lots and lots of doors.
NARRATOR: During this time, our neural circuitry gets fine tuned.
TOTTENHAM: Our brain learns about which connections are going to be important through a use it or lose it principle.
PASCUAL-LEONE: Certain connections become reinforced and sustained and enhanced at the cost of others.
TOTTENHAM: Those connections that aren’t being activated because they’re learned not to be necessary, get pruned away.
NARRATOR: They actually die off, and the open doors begin to close.
PASCUAL-LEONE: As an adult, if you’ve never played, you’ve lost that door.
NARRATOR: So right now, Augie can learn to speak any human language perfectly without an accent, but when he’s an adult, he will have lost that ability. If he doesn’t begin learning the violin before he’s about seven years old, he’ll probably never play Carnegie Hall.
PASCUAL-LEONE: If you never had the connections to begin with, you can dry as hard as you can. You’re never going to get there.
NARRATOR: But what if we could change that? What if we could tweak our brains to learn as easily as a child? It’s called The Holy Grail of Neuroscience, and it is tantalizingly close.
PASCUAL-LEONE: We can, to some degree, do the impossible and reopen critical periods to say we allow changes to happen later on, in ways that we didn’t anticipate would be possible.
NARRATOR: Scientists are learning how we learn, and that may soon give us a chance to reopen those doors.
GUY MCKHANN: So what actually is neuroplasticity? Neuroplasticity is the ability of the brain to adapt to changing circumstances. To an environment changed, the ability of our brain to in a nutshell learn. But there’s another side of the coin. Just as we need to be able to learn to adapt, we also need stability. The opposite of plasticity, neuroplasticity, is brain stability. So in fact, that balance is what we’re going to focus on a lot tonight.
MCKHANN: Our first participant was the first woman to chair the Department of Neurobiology at Harvard Medical School. Today, she’s professor of Biology and Neurobiology at Stanford University. Please welcome one of the world’s foremost neurosciences, Carla Shatz.
Our next participant is Associate Professor of Psychology at Columbia University, director of the Developmental Affective Neuroscience Laboratory, Please welcome Nim Tottenham.
Our third participant this evening is Professor of Neurology at Harvard Medical School. An MD-PhD, he says his research falls in the area between the brain and the mind. Please welcome Alvaro Pascual-Leone.
MCKHANN: So welcome everybody. So Carla, let’s start with the brain itself. We’re going to be talking about learning plasticity, how the brain learns, how skills become habit. But what do these things actually look like in the brain structurally?
CARLA SHATZ: We saw already some nice photographs in the introduction, if you remember of these black things. Structurally, the brain is composed of neurons and support cells. The neurons communicate with each other through electrical signaling; chemical electrical signaling. The most important aspect of that is that these communications are transferred across structures known as synapses. That’s where learning happens. That’s where memories are stored, and as we were talking about in the video, that’s where the pruning, this pruning process goes on, this use it or lose it process goes on during development.
So, in fact, the structure of the brain is just the brain is packed with these neurons, packed with these synapses and also with very long connections. Some of those you can actually see in this beautiful graphic that’s being displayed now. So the brain connections link various parts of the structure to each other, ad those are the beautiful colors that look like Us and so on, these pathways. But those are made up of hundreds and thousands of connections from individual neurons. I used to joke there are more neurons in the brain than stars in the universe, but in fact, an astronomer corrected me and said that wasn’t true.
MCKHANN: So when you look at an amazing picture like that, we’re looking really at the axons, the wiring-
SHATZ: The wiring.
MCKHANN: Is the brain fundamentally un-wired at the start?
SHATZ: The brain is not fundamentally un-wired at the start. But it is amazing, if you just take the visual system, for example, the eye is not connected to the brain to start with. The nerve cells in the eye, have to grow their connections along pathways and select the right part of the brain, namely the visual part of the brain, not the auditory part of the brain or the motor part of the brain.
So the wiring from the very beginning is very highly organized and the formation of these long tracks or pathways is dictated by very strict cues like pathways or even like roads with street signs on them, so that these growing connections or the growing axons follow these pathways. But then the amazing thing is once the connections form between these long distant regions of the brain, then there’s this period of overproduction and pruning that we’re going to talk about. A period of extensive plasticity where the outcome is really predicted by the use of the circuit itself and the experience itself. So there’s both directed kind of hard wiring early, followed by this remodeling plasticity that happens later and really persists to some extent throughout life.
MCKHANN: So then building on that, if we think about it, if you’re building a house, you’re not going to lay copper wires all over the place and then pull out the ones that don’t seem like they’re working well. But that seems to be what we’re talking about. It seems pretty inefficient and the brain is 2% of the body weight, but yet gets 20% of the blood flow and 25% of the glucose. So why is the brain doing it that way?
NIM TOTTENHAM: Yeah, so on face value, there’s so much about brain development that seems inefficient, but actually it’s that seemingly inefficient path that actually gives rise to the incredible complexity of the brain, especially in the case of the human. So when we’re developing, what our brain does is first goes through this period of over producing our neurons and synapses and then through experience, through learning what’s important in the environment, what synapses are getting activated, those get to stay and everything else gets snipped away because it’s inefficient to keep all of those synapses.
So, why would we go through this entire process of over producing and then pulling back? That’s really at the core of what the function of childhood is in the human. So if you think about humans as a species, we’re amazing in many ways. We can live anywhere on the planet. We can speak any language, we can eat a number of foods and so on and live very well. Some of the reason why we can do that is because of this long period of brain development that we have. So the brain overproduces, it’s like throwing a big fishing net out into the ocean because you’re not sure which house you’re going to end up in. You’re not sure what language people are going to be speaking to you.
So you’re ready, you’ve got all your bases covered. Then depending on what signals are coming into the brain, the brain learns, “Okay, I’m going to keep the synapses, but I’m going to get rid of these. So if I’m growing up in a Japanese speaking household, I’m going to hang on to the synapses that help me understand Japanese, but get rid of the synapses that support other languages because that’s really efficient.” So it really is this developmental period, a really long one in humans, that gives rise to our incredible adaptation to our particular environments.
MCKHANN: So, Alvaro, is this a new concept? We all think everything’s been figured out in neuroscience in the last 20 years, but this need to balance stability and plasticity, tell us a little more about that, about the history of that conceptual.
ALVARO PASCUAL-LEONE: I think there’s lots of new developments, but many of the ideas are not fundamentally new, we have the tools to actually test the concepts. But the first person to speak about plasticity and stability as a term and apply to behavior; to human behavior, was Williams James; the psychologist Williams James in the 1890s. He wrote about plasticity as being the property for substance of an organ, presumably of the brain, that enabled us as humans to do certain behaviors and become really good at it. He was talking about behaviors, a habit, not about the brain structure. He said, the amazing thing, it has a property of giving in to influence but not giving in all at once. You want to have some plasticity but not too much plasticity. You want the right kind of plasticity, the right amount of plasticity.
Presumably, it was Ramonica Haldane, not much longer, who started to look into where does that actually happen in the brain and describe the synopsis and the changes in the connectivity and the change of how efficacious those connections were in making new ones as the substrate for that plasticity that Williams James was talking about. So the ideas are 100 years old, and yet when I was studying medicine, I was told, “Things don’t change in the brain and when you get old, well tough.” I thought, God, I hope we can do something about it because I hope to get there one day.” I think we start and all know, we’ve always known, as an old dog, you can still learn new tricks. It was against the experience of everybody that it is possible to learn new stuff. So how does that gel together?
MCKHANN: Great. So now let’s go back to this. We were talking about this concept of a critical period. We all know the old adage that children learn language a lot more easily than adults. But what are some of the other examples of critical periods that you see in your work with children?
TOTTENHAM: So for a while, people were thinking that there is a critical period of human brain development that was the language that people used and then it became clear that critical periods are really a property of a developing neural circuit. So if that’s true, then maybe it’s appropriate to think of each neural circuit that we have as undergoing its own critical period. That moment, the metaphor that people often use for a critical period is that it’s a window of opportunity opening up when the environment can really have its biggest impact on the nature of future functioning for that system.
If it’s true that every neural circuit has its own critical period, then maybe we can sort of map out the timing across the brain. So in general, what people find is that the brain develops in this backwards C-shaped nature where regions of the brain that are low and back tend to develop earlier, then the development curls around in waves.So what you often see, sensory systems develop earlier, experience their critical periods, followed by motor systems and language systems, and finally more of these higher cognitive functions that particularly in the human, we spend so much time thinking about. So, things like our emotion processing or our cognition, academic performance and so on. So, that hierarchical structure really makes sense when you think about what the needs of the developing infant child or adolescent are going to be.
MCKHANN: So the video, we saw a baby turtle that really doesn’t have a childhood. It jumps in the ocean and takes off whereas humans, we have this extended childhood period where all of this has to happen. You could argue that because we have the most to go through experientially, that we have the longest childhood.
TOTTENHAM: I think it’s another good example of what seems like an inefficient design, right? So if we’re going to stay and mature for that long, then we need somebody around us who’s willing to put in the investment to stick around with us that long. So if you look at this immature period in the human, it’s really a long time, right? In most species, this period of immaturity is on the order of weeks, maybe months. In humans, it’s years.
So that’s a curious design from mother nature to come up with because it’s a huge energy suck for a parent, right? To raise another human being. I don’t remember, I don’t know what the numbers are, but someone computed how many calories it would take to raise another human being and it’s enormous. So there’s gotta be a really big payoff. One of the arguments is that the payoff is that this affords us as a species, this incredibly long period of plasticity so that we can do all the learning that’s necessary to become a very complex adult.
PASCUAL-LEONE: So at the same time, I think what we’re learning is that there’s this notion of development and then you get to some level of maturity, which I’m still hoping for, and then you have a plateau and at some point things go wrong and if you are unlucky, you start losing it. This way of thinking about it is probably the wrong way to think about it. That, instead, we should think of us developing our entire lifespan until we sort of die and that therefore plasticity, even though it may be through different mechanisms and different efficacies and working on different substrates, but it’s still there.
It’s still there throughout the lifespan. So it’s not a critical period in the sense that plasticity is done and now you can reactivate plasticity. You can open opportunities, but the capacity of change, balancing the stability is there for the entire lifespan, which is from a neurologist’s point of view or neurosurgical perspective, a huge opportunity and reason for hope and of interventions.
SHATZ: This balance between stability and plasticity is really interesting. If you just think about some of the systems that have to form, then you don’t want necessarily plasticity throughout life in a system, let’s say, like our visual system where we need to have a stable representation of the world inside our brain. Then we can draw upon that to make computations to put together and to have perceptions and so on.So it’s really quite interesting. So some systems really need to go through this learning period, but then to become more stable than other systems.
MCKHANN: So let’s let build on that a little Carla, because the visual system, your mentors at Harvard, Hubel and Wiesel won the Nobel prize in 1981 for their fundamental work on really the first insights into all this concept and the visual system. So help us understand that a little more.
SHATZ: Oh, sure. So, this is David Hubel and Torsten Wiesel. My mother … I used to call them Hubel and Wiesel and my mother thought it was a person, one person Hubel and Wiesel, till she met them. But yeah, so these two wonderful scientists explored the visual system and began to try to understand how it is, well, here’s the question. How come we see with one view of the world, even though we have two eyes?
So both eyes have complete circuit. It’s like you have two cameras. I mean, both eyes bring complete images of the world to the brain, yet unless there’s pathology, we only see one view of the world. The answer to this as both in the wiring of the connections and also the fact that the brain has to learn how to use both eyes together. It does that during a developmental critical period. So the connections from the two eyes begin to be mixed together as the connections move from the periphery, from the retina itself into the central nervous system. The first binocular cells are actually built in at the back of your brain in your occipital cortex. That’s your primary visual cortex.
But even though the connections know to grow to the visual part of the brain, they actually don’t know how to tune up to make binocular neurons. One way they do that is to interdigitate the connections between the right eye and the left eye into a series of beautiful right eye, left eye, right eye, left eye stripes. You’ll see two images here actually. So there’s an image where there are white and black stripes and those stripes are equal in size-
MCKHANN: On the left.
SHATZ: On the left. Then there’s another image on the right where there are little teeny black holes in the middle of a sea of white. Now what you’re looking at, let’s just say on the left, every little white dot is the size of about a synapse. So one of these connections and you’re looking then at literally millions of these connections. What you notice is that they’re beautifully organized in the stripes. When Hubel and Wiesel first discovered this intermixing of the two inputs, which are essential for making the binocular neurons, everybody thought they were hardwired.
But they did a very important experiment. The experimental result is on the right. Let me tell you about it in just one other context, which is really to talk about the mystery of the cataract. So you know perfectly well if as an adult you have normal vision your whole life and you get a cataract as an adult, you lose the vision in your eye because there’s a clouding of the lens. Then a miracle can happen. That you go to the surgeon and he replaces the lens with a clear lens and you see beautifully again, immediately. This replacement could happen after maybe 10 years of not being able to see well through your eye.
Now, in contrast, a little child who might be born with a congenital cataract or have some other problem with vision in one eye, if that cataract is not a corrected immediately, then that child will be permanently blind or have severe vision loss in that eye. So what’s the difference? My grandma had a cataract, 10 years worth, corrected, good vision, and then the child maybe has a cataract just for a year, maybe even half a year, and it’s corrected, the optics of the eye are corrected, the camera works, but the brain can’t see. So what’s the difference? Hubel and Wiesel did an experiment where they actually checked the connections between the eye and the brain that was shown in the right hand side.
The open eye, the white eyes connections take over way more than their fair share of cortical circuitry for vision. The closed eye has those little piddly black holes. This was an amazing demonstration, a very important demonstration, in fact, the first of the use it or lose it concept in the brain. That the brain connections require use in order to be maintained and in fact even require use in order to be formed.
MCKHANN: So can you go into a little bit how you’ve been building on that work? I think you’ve got a video for us of how the brain does this in real time?
SHATZ: This really illustrates a developmental critical period that happens after birth. But actually, we were quite interested in knowing whether there are earlier developmental critical periods in the visual system. What we discovered is that even before babies are born, the eye is sending signals to the brain to start to really shape up these beautiful stripes and these connections in the central pathways. The signals are the electrical signals that are being sent from the neurons in the retina into the central part of the brain. They’re actually like test patterns, they’re at testing the connections, and the ones that are appropriate are being maintained and the other ones are being pruned away. So this is the same theme.
The video that you see now is a picture of that signaling process in the eye. So you can just imagine it’s like phone calls being placed to the brain really early in development and every little black dot here in this video is again about the size now of a nerve cell, not a synapse. So it’s a bigger scale, but you can see that whenever … when the cells become black, it means they’re placing the phone calls and they’re sending their signals to the brain. So, what you’re seeing here is neighborhoods of nerve cells, all placing phone calls together.
This is actually part of another principle of development, cells that fire together wire together. So this is a way that the eye can test to make sure the connections are orderly in the target structure. This is happening. So the brain is really jump starting vision even before vision is possible because it’s in utero, and it’s before the rods and the cones have appeared. Now that we know that this happens in the visual system, it’s been found that this kind of jump starting and testing is happening all over the brain during development, very early development.
MCKHANN: You’ve been studying ways to potentially reopen the visual system. So tell us about that a little bit.
SHATZ: Yeah. Well, the question is really if these windows close, can you open them up at any time? And really to try to understand how to do that, it’s important to know something about the molecular mechanism. So what are the molecules that are opening and closing these developmental critical periods? And really in particular, what are the molecular mechanisms that control the pruning process itself, this selection process, which synapsis should we keep? How does the brain know that certain synapses have been used and they should be strengthened and other synapses have not been used so much, so we don’t need them, so we can actually prune them away?
So we can use animal models to begin to discover those molecules for pruning. In doing that, in fact, we found a number of candidate molecules that we wanted to test to see if they were important for this pruning process. We engineered genetically mice that lack these molecules to see what would happen to their critical periods and to pruning. To our great surprise and delight, what we discovered is that if certain of these molecules, when they’re not there, permit the persistence of the developmental critical period in the visual system and in fact pruning fails to happen. So this is illustrating two points. One is that it is possible to continue to extend a critical period for a longer period of time. It also indicates the idea that brain plasticity itself can be regulated in a very deliberate way, and if we only knew the whole story about the molecular mechanisms, we really could make pills and I could take a pill as an adult and learn French without an accent.
MCKHANN: So that brings up an interesting point because Alvaro is over there smiling and shaking his head. So as a clinical neurologist-
PASCUAL-LEONE: I’ve taken the pill, exactly.
SHATZ: No, but would you want to take it right away?
MCKHANN: As a clinical neurologist and you think about that and we talk about the balance between stability and plasticity and as you’re taking care of patients with strokes and things like that, what do you think about in kids as … Well, ’cause everybody’s obviously going to, “Well, we got to get these into humans. We’ve got to figure out ways to extend these windows for kids and for disease to adults.” So let’s talk a little bit about the pros and cons of that.
PASCUAL-LEONE: Yes, I think it’s a really important topic and it is a double edged sword. So to have a great efficient plastic brain that is able to get us to learn French or English without an accent, it may be very appealing. But at the same time to have too much plasticity can come with a cost. If you have, not in a genetically engineered mouse, but a disease where by design, because of their pathology, the brain is too plastic, is learning too fast, and that seems at face value a great thing. You’re able to acquire skills that go above the average one of us.
You can open up a box of matches, have them fall on the ground and say 27 and be right or 225. You can learn a whole book of names and phone numbers and we call those savant abilities. It’s sort of cool and it’s certainly partly a joke. But it comes to the course because what happens to the brain is that normally it yields to influence to the environmental change. Then we stop and then we experience a new thing and that new thing falls on to fertile grounds, ready to learn the new thing. But it doesn’t get colored, but what we just learned.
The risk of having too much plasticity is that the brain is change and then the change falls on to the change and the change into the change and the change … it is often a messy, noisy system. We think that for example, diseases like autism are characterized by excessive, too good at plasticity, that leads to a failure of pruning and to a developmental disorder because of the number of [inaudible 00: 35: 24] plasticity. So to have too much may be a bad thing.
MCKHANN: So you’ve been studying that in autism specifically to try to look at plasticity in the autistic brain versus in the neurotypical non autistic brain. So what do you find, how do you go about teasing that apart and what do you find?
PASCUAL-LEONE: You have to come up with experiments is it worthy to show that people with autism can be better at learning for example than the individuals that are not autistic? And things like learning a sequence of finger movements that repeat themselves by doing it to figure out the pattern underneath the finger movements. Individuals with autism learn to do that faster than those without autism. But if you have one pattern followed by another, then they break down because they run into interactions between the two things that they are learning.
At the same time, we want to look in the brain and see what is changing in the brain to allow them to learn these skills faster. We do that in a similar way, that we’ve learned to do it in animal models or in slices of the brain using electric stimuli to evoke a response and then using trains of little stimuli to modify those connections and see for how long they remained modified. We use that using a technique called transcranial magnetic stimulation.
MCKHANN: So tell us a little more about that technique and how you’re able to use it noninvasively to test something like this. To perturb the brain transiently.
PASCUAL-LEONE: It’s a bit like science fiction. It’s still to me. You basically put a coil of copper wire over the subjects head then as the current passes through the copper wire coil, it induces a current that goes through the skin and the skull and induces a current in the brain. Maybe we can show it and it has a little explanation that goes with it.
NARRATOR: TMS stands for transcranial magnetic stimulation. It is a way of inducing current in the brain. You need specific controlled part of the brain without having to open up the skin and the skull. It turns out that when you apply repetitive stimuli, then you’re activating a zero grid over and over in your control pattern, and that changes that [inaudible 00: 38: 07] zero grid. So that allows us to activate, probe, disrupt or suppress activity in different parts of the brain depending on where we target and what parameters of stimulation we applied.
PASCUAL-LEONE: So you can probe the brain with this technique, see the response, apply a little train to modify it. Then what you find in people with autism is that the effect of that modification lasts literally longer than it does in neuro-typical subjects in those without autism.
MCKHANN: So Nim, we’ve talked mostly and now we’ve talked about vision and we’ve talked about motor system. You study a lot more aspects of emotional phases of development. So let’s talk about how you’ve been studying that in these exact same context of plasticity and stability.
TOTTENHAM: A lot of our questions are related to the point I made earlier that we have this design of spending a lot of time with our parents while we’re growing up. So we have been very interested in the role of the parents during this putative sensitive period for emotional behaviors. So, we know since the time of Freud, that there is this very strong association between early caregiving experiences and emotional behavior later on in adulthood. But we don’t really know at the level of human brain development why that enduring link exists. Part of the answer may have to do with some of these critical period timing and the influence of the parents. So we’ve been asking questions about, actually, what good is a parent? We know that parents are important, but what are they actually doing on a moment to moment basis? As I’m rushing my kids out the door to school, shoving breakfast into their mouths to get them out the door, what are those momentary episodes important for?
But we also have the opportunity to ask questions about children who experience more forms of adversity early in life. The reason that we’ve been very interested in this group of children is because this early adversity exposure is one of the number one preventable risk factors for emotional difficulties later on in life. We’re just at the beginning stages of understanding why early adversity in particular is so important, maybe more important than later adversity. Part of the answer is related to the concept of critical periods that we’re talking about.
So you brought up the idea of a double edge sword before. I think that there are many double-edged swords when it comes to brain plasticity. Another one of those is that brain plasticity is not really good or bad. It just is. It just opens you up to the environment. So when considering or evaluating brain plasticity, it’s also important to look at what’s the nature of the environment that the individual is experiencing when the brain … when that window of opportunity is really open.
So for children that have experienced significant adversity, like caregiving adversity or what we often call psychosocial trauma, what we have seen, well, two main things. One is that there’s incredible individual differences in outcomes. So some children show some really significant challenges and others are thriving. So this is an individual differences story that we really aren’t very good at explaining right now.
But the other piece that we’ve been seeing, and this is true not only in humans but across a number of species, is that early adversity may actually be affecting brain development on average by affecting the timing of these critical periods. So there may actually be an acceleration of the timing or the opening of these critical periods. So if we know that, that’s really important to know in terms of intervention and prevention, because if the timing of these critical periods are shifting as a function of early experience, then that informs how we want to treat individuals and what new experiences we want to give to individuals as a function of these early experiences.
MCKHANN: And that’s why you like to refer to these, as you said before, as sensitive periods, more than critical periods.
TOTTENHAM: For the processes that we’re interested in, these emotional behaviors and cognitive behaviors, that seems to make more sense to me because they do seem to be more malleable. In fact, that’s why talk therapy is supposed to work. Is that talk therapy is about teaching the brain something new about interpersonal relationships. The reason, the only way that talk therapy can work is if there’s continued plasticity in some of these systems.
MCKHANN: So we talked a little bit about autism. Let’s talk a little bit about schizophrenia because they’re another very complex condition and there are questions about whether or not schizophrenia may have aspects of a disorder of stability and plasticity. So, Carla, maybe you could enlighten us on that a little.
SHATZ: Well, I mean, one main point to make about schizophrenia is that it’s not really commonly considered to be a developmental disorder. Even though often symptoms appear late in late adolescence or even beyond, the current idea is that there’s this extended developmental critical period and this period exists beyond the visual system as Nim has mentioned.Therefore, these systems that are maturing much later, including those that have to do with interactions and with cognition and frontal lobe behavior, all mature later. So then the question is what are the changes that have happened in the brain?
Again, it’s commonly now thought that this relationship really between plasticity and stability must be perturbed in some way. When people look into the brain of a … not a huge amount has been done, but there is consensus that there are changes in pruning in the brains of schizophrenic patients who have donated their brains for studies so that we can actually look at those brains. In human genetic studies we’re looking for susceptibility genes that might produce schizophrenia in children, some of the new gene candidates that have been identified are known in animal models where we study how those genes actually work, are known to regulate pruning in the animal, like the mouse developmental critical periods.
So, now you’re beginning to hear a kind of common theme that’s emerging as we talk, that there are these critical periods that involve a beautiful balance between plasticity and stability, involve pruning and may have different outcomes, not only through our own experiences, but also when the balance somehow is disrupted by some kind of pathological condition.
GUY MCKHANN let’s talk a little bit about how do we harness recovery of damage after injury. You talked a little bit, Nim, about a traumatic situation, but what about critical periods in childhood, when we get to adulthood, how do we attack that problem?
PASCUAL-LEONE: Well, I think the way we’re talking about plasticity really say it’s a huge reason for hope, right? It suggests the fact that our brain can be guided and the challenge is to learn exactly how to guide it. What do we need to do to suppress changes that are these double edge sword that good cause problems and to enhance others that can benefit the subject? We have lots of interesting indications that that is possible to do. Ultimately, that’s what physical therapy, what occupational therapy, what speech therapy promotes. Is the talk therapies guide the changes for the benefit of the subject.
But I think we have now as we understand more of the molecular basis and the physiologic basis of these mechanisms, we have ways to target these mechanisms with medications or with devices, with brain simulation that more directly to the brain promote the changes. That’s happening and it’s happening guided by basic research and translating that basic research to humans. So … sorry.
TOTTENHAM: One of the things that I’m really excited about in terms of intervention is thinking about how can we boost the power of current interventions by knowledge about critical periods in plasticity? So if we can increase plasticity prior to some known effective intervention, that’s really powerful. So, as you mentioned, there are many examples in basic neuroscience where pharmacologic or genetic administration or modification can actually increase plasticity, and in many ways, bring the brain back to that childlike state to allow for some environments to have a really big effect on the brain.
That’s really powerful and there’s a demonstration in humans too that has actually used one of these pharmacological manipulations with people who don’t have perfect pitch and perfect pitch depends on critical period learning early in development. So perfect pitch was able to be developed in adults who had taken this pharmacologic drug. So then the question is, well, why don’t we all do that? Right? The authors of the study make a really … they’re very careful to say that, “Hey, remember the brain actually spends a lot of energy to prevent these critical periods from opening up again.”
The brain wants efficiency, the brain wants reliability. Do we want to remove all of the lessons that we’ve learned throughout our entire developmental history? Do we want to remove aspects of our personality and so on? So it becomes a very tricky question even though there’s a lot of promise for recovery following any type of trauma.
SHATZ: But in that perfect pitch study, they didn’t … the people didn’t lose … I mean, they learned something new. So there’s hope really. There’s hope for having a selective intervention. I think that’s exciting. I mean, from the animal studies. So, from looking again at the mice … and actually one of the authors of that study also has done work looking at the mouse critical periods for vision as has my own lab.
What we find is that you can actually go into the adult mouse brain and really restore juvenile plasticity in the adult brain. The mechanism of doing that seems to be, again, to allow for new synaptic connections to form. If we study the story of the childhood cataract, but now in the mouse, then remember I told you that if children have a cataract and it’s not immediately operated and, and clear optics restored, then they become either permanently blind or that vision is seriously diminished in that eye.
And really there isn’t a good way of treating that blindness, is called Amblyopia, in adulthood. But in these mice, one can actually make the cataract model and then go in the adult mouse, and engaging these childhood mechanisms of plasticity a effect recovery of vision in the eye that was blind, which is amazing. It’s really … demonstrates, I think, that by understanding the underlying mechanisms that regulate these developmental critical periods, it’s possible to go in and then to manipulate them again. To me, it demonstrates another thing, which is that there must be in the adult brain and presumably in our brains too, ’cause we have the many of the same molecules that are being studied in the animal models, there must be brakes on plasticity because these manipulations essentially take the brakes off and then of course you can worry about stability.
So then we come back to that, this whole theme. Again, but the idea that there’s actually more plasticity in our adult brain that we can tap into, to me is really exciting because you could say that even if there are some downsides, that after a stroke or damage to the brain, wouldn’t it be wonderful if it were possible then to tap into that latent extra plasticity even briefly and combine it with training and physical therapy. So somehow a pill that would let me speak French without an accent could actually have a really important therapeutic value, which would be to really help people recovery from brain damage.
MCKHANN: Well, what we have here is a video of a modern rehabilitation technique with a split treadmill. Maybe, Alvaro, you can tell us about the concept behind this.
PASCUAL-LEONE: Yes. So part of what physical therapy interventions like this or like something called constraint therapy that some of you may have heard about it in individuals that have stroke, that cannot use both legs in walking correctly or cannot use one hand correctly, we’ve come to learn that if you force the use of the other hand, of the impaired hand by limiting the default of just using the unimpaired hand or by in this case of the video, if you force the walking correctly by aligning the paretic leg because it cannot cross over, so, therefore limit the pattern of abnormality that normally would happen, that because of this repeated training doing the right thing, that promotes the rewiring that promotes the plastic change and speeds up the recovery.
So you can, by guiding, by constraining the behavior, use that as a way to improve the recovery process. So the opportunity of opening up the mechanisms of plasticity in such a way that they become more active and therefore benefit from the intervention more, becomes really appealing. Examples of that do exist even in humans, not only with medications. One of the things that we know about Alzheimer’s dementia, Alzheimer’s disease is that before the clumps of this abnormal protein come together and deposit the plaques in the brain, they are floating around. In that stage already they alter and damage synapses. So they become damaging substances for the mechanisms of plasticity as it were. If you take patients with Alzheimer’s disease and you try to get them to learn from video games or computer games and get better at cognitive tasks, they derive very little benefit. It would take too long to get a benefit that is sort of meaningful.
But if you activate that zero grid with brain simulation, for example, just before they actually engage in the cognitive training, now you get more benefit from the cognitive training. So combining interventions, device base pharmacologic interventions with behavioral interventions, I think is really a way to leverage what we know about the mechanisms of plasticity in a way that translates into benefit for patients.
MCKHANN: So we’ve talked a lot about aspects of disease and repair. What about this Holy Grail idea? What about the idea of actually enhancing the brain? Whether one day I was thinking, “Today, I had a long day,” and I was thinking, “Oh my gosh, I got to focus on what we’re doing tonight,” and I jumped in a car and when is the helmet going to come out through the ceiling or already being built into the roof where I can say, “If I can just get my temporal lobes going and my memory working a little better, how great that would be.” How far off are we? How far off are we from everyday enhancement of function?
PASCUAL-LEONE: It didn’t work this morning exactly.
MCKHANN: You were in the wrong car.
PASCUAL-LEONE: I was in the wrong car. I mean, what gave me pulse is that of course there is a lot of industry investment and really direct to consumer devices already claiming that that’s possible, that we don’t need to wait at all. That you can just do it today and you can build your own brain stimulator devices and then build it into your car if you want to. People will claim and try to convince us that it is possible to enhance capacities. The problem with a lot of those data is that what they show is that it’s possible to get better at performing a given task, not to actually get better at the fundamental skill that underlies the task.
So, I think that the attempt to get us there is already here, but we need greater understanding including greater understanding of that double edge aspect that Nim was mentioning.If we get better at one thing, will it be without a cost? Will the brain allow you to improve something at the cost of something else. So, for example, you can ask a question and say, “What if we were able to get better at paying attention to this part of the world? We know a lot of what the circuitry is, that allows us to pay attention to this particular spot.”
So you can actually identify those brain areas in humans, apply simulation that increases activity in those brain areas, and you can make people get better attending to this part of the world. But when you do that, it comes at the cost of attending to this part of the world. In fact, it does so because these two areas sort of … I almost say it is a yin yang kind of a relationship.So there are interactions between the two hemispheres. So if you improve one, you worsen the other. That’s easy to test in something as concrete as spatial attention for a visual task and something that’s complex as overall behavior or more higher order cognitive functions. What exactly the cost might be, is much, much harder to test. I think it raises not just methodological and biological questions, but real ethical questions. If you want to improve certain skills, what would potentially be the downside of it?
MCKHANN: What about memory? I mean, memory is something … to varying degrees, we’re all here, slowly moving along chronologically and everybody worries about what’s going to happen to your memory. In my world, people have the ability to sometimes put electrodes into the brain. That allows us to stimulate the brain and there’s a number of reports of different parts of the brain, if you stimulate at just the right way, you can make somebody’s memory performance better.
How do you think of that, as not a way to combat aging per se, but to help people adjust as they get older and keeping memory intact? Forget about super memory, even just trying to keep memory intact as we go along. How do you guys see us approaching that?
TOTTENHAM: I mean, correct me if I’m wrong, but aren’t there less sexy, innovative ways that people think about or have studied to enhance some of these processes? So, for example, the things that we know we should do, like getting good sleep, exercising. Engaging in cognitive stimulation throughout a lifetime have been associated with better cognitive aging in the long run. So those are hard things that we all know we should do, but routine things that we should be doing that may actually be improving some of this retention over the long term.
PASCUAL-LEONE: So lifestyle modifications do work and do work through plasticity. So physical exercise promotes cognitive function. In fact, if you do an analysis of all the studies that have been done in the literature which we just did, just published in … there is a … I don’t know why this is the number, but there is about 52 hours a day, 52 hours …
MCKHANN: Talking about enhancing…
TOTTENHAM: It’s really hard work.
PASCUAL-LEONE: It’s really hard work. 52 hours in six months actually. So it’s not a lot and it doesn’t matter how many hours per day you do it, it’s sort of a total amount of dose almost. But you need to put in some hours but it’s not a ton of hours-
TOTTENHAM: Of exercise?
PASCUAL-LEONE: Of physical exercise that improves cognitive function in the elderly. So I think that there is an effect of physical exercise onto the brain and it appears to be linked to mechanisms of plasticity, at least as one can probe them in humans with brain imaging and brain stimulation techniques. But I think rather than getting at the level of suggestions, you should sleep better, avoid medications that are bad for you, eat the right thing and the right amount and exercise and challenge your brain with new things and have social relationships.
All those things are true, but we should be able to get to enough understanding that we can prescribe it, that we can tell men, “This is the number of hours of this exercise that you need to do and here’s how we’re going to help you actually convert this hopes into realities.” Because it’s hard to stick with a program like that. So I think that’s the step that we still don’t have, is the understanding of how to actually make this a prescribable intervention, like we do with medications. We don’t tell patients, “Take something for that.” We tell them what to take and how much and so forth. So I think we need that level of understanding.
MCKHANN: But what about, Nim, happiness set points? Everybody wants wellness. Is it possible that we’re going to someday understand the brain well enough to say, “Okay, you’ve been through a really terrible life trauma, but we can actually help your set point.”
TOTTENHAM: Well, I would think about sort of maybe not happiness, but that feeling of being able to regulate your emotions, to be able to feel less sad when you want, to be able to feel more sad when you want. To have that emotion regulation ability. So there are studies, for example, with people who meditate, which we generally think of as a healthy lifestyle practice. But there are different levels of expertise in meditation. So there are Buddhist monks who do this for, say 40,000 hours in total versus really, really dedicated meditators who might’ve done this for 20,000 hours, and then novices. This research has shown that the amount of meditation practice, practice being the keyword, that the behavior has to be routinely engaged with, is associated with brain changes in the regions of the brain, like the prefrontal cortex that we know are associated with emotion regulation.
What’s interesting in that finding, and it relates back to the original walking example and the quote about habit, is that there was this inverted U-shaped dose response function such that the individuals who were meditating a lot but not to the degree of the Buddhist monks actually had the most different prefrontal cortex activity and then it came back down again for the Buddhist monks, suggesting that there is this element of plasticity in the brain regions that we know are associated with emotion regulation, but an element of habit can come into play as well, so that it starts to become more of a naturally occurring state of the brain that can be, as you were referring to before, the core process that’s being affected rather than the more superficial.
MCKHANN: So I would have to say in summary, that obviously we have a really, really tight balance between plasticity stability. But as we’ve all learned, they’re incredibly exciting things, not just normal behavior, attacking diseases going down the road.
But in the meantime, eat well, sleep well, meditate once in a while, exercise a whole lot, and surround yourself with really smart people who make you happy. For that, I thank all of you.